Royal College of Physicians issues stark warning over social care crisis
By Gabriel Blaazer
The Royal College of Physicians is warning that the combination of an ageing population and a lack of NHS workforce planning means the country is risking an unavoidable crisis in social care for older people.
The Royal College of Physicians (RCP) has issued a stark warning that NHS workforce shortages are driving the social care crisis in England and that the NHS is “woefully unprepared to cope with an ageing population.”
New analysis from the RCP shows that there is the equivalent of just one full time geriatrician per 8,031 people over the age of 65 in England. The findings use data from the RCP’s own census of physicians and the Office for National Statistics’ (ONS) population data and demonstrate the extent to which England’s care crisis is only set to grow.
The ONS estimates there will be more than 17 million people aged 65 and above in the UK by 2040, meaning 24 per cent of the population would require geriatric care. Additionally, many of the doctors currently providing geriatric care will, themselves, soon be requiring the same care, and 48 per cent of consultant geriatrics are set to retire within the next 10 years.
Considering these trends, the RCP, along with more than 100 medical organisations, is supporting an amendment to the Health and Social Care Bill requiring the government to publish “regular, independent assessments of the numbers of staff the NHS and social care system need now and in future.” No such data is currently publicly available. The amendment, currently being debated in the House of Lords, was tabled by Baroness Cumberlege and is supported by former NHS England Chief Executive Simon Stevens (now Lord Stevens of Birmingham), is set to be debated in the House of Lords
Responding to the RCP’s warning, Danny Mortimer, Chief Executive of NHS Employers and Deputy Chief Executive of the NHS Confederation, said: “As exhausted NHS staff strive to tackle the enormous treatment backlogs that have resulted from the pandemic, we must not forget about the pressures that our health and social care services face as they work to meet the growing needs of our ageing population.
“To be able to plan effectively for a future workforce, healthcare leaders need clarity in the shape of a clear long-term workforce plan. Sajid Javid’s recent commissioning of a workforce strategy is a very welcome step, but… we would urge the government to accept amendments requiring the health secretary to publish regular, independent assessments of the numbers of staff the NHS and social care system need now and in future.”
The President of the RCP, Andrew Goddard, said: ““I have dedicated my career to working in the NHS – a service that I am fiercely proud of – and yet it scares me to wonder what might happen should I need care as I get older. There simply aren’t enough doctors to go round, not least within geriatrics.
“The workforce crisis we’re facing is largely down to an astonishing lack of planning. All successful organisations rely on long-term workforce planning to meet demand and it’s absurd that we don’t do this for the NHS and social care system. The government needs to accept the amendment put forward by Baroness Cumberlege and make workforce planning a priority.”
Dr Jennifer Burns, President of the British Geriatrics Society, said: “These figures show very clearly the current nationwide shortage of geriatricians – a situation that will only get worse with the predictable rise in the numbers of older people across the UK needing healthcare.
“It is absolutely vital that these fundamental issues around the recruitment, retention, development and support of the workforce are addressed, and that there is a properly-resourced strategy for future needs. The British Geriatrics Society stands with the RCP in strongly supporting the amendment to the Health and Care Bill.”
New IPPR report argues health is ‘holding back UK economy’
By Niamh Macdonald
The UK will suffer an £8 billion hit to economic activity this year due to lack of government action to improve the nation’s health, according to a report launching the new cross-party IPPR Health and Prosperity Commission.
The IPPR report published today marks the launch of a new Commission on Health and Prosperity. The report warns that health inequalities and ineffective policies are shortening life expectancy in the UK, coupled with more years spent in poor health.
New analysis by IPPR and health analytics company Lane, Clark & Peacock, reveals that the workforce is also being affected as people face barriers to staying in work.
The IPPR is calling for a ‘new post-pandemic approach’ to the nation’s health to ensure that people can live long healthy lives as well as to strengthen the UK’s suffering economy.
There are now more than a million workers missing from the workforce compared to pre-pandemic levels. About 400,000 of these individuals are no longer working due to health factors, including long Covid, disruption to healthcare and declining mental health. The researchers warn that without intervention, this will drag down economic activity this year by approximately £8 billion.
The report states that the relationship between health and the economy is a decisive factor in the UK’s low productivity, low growth and significant regional inequalities.
According to the report, local level analysis reveals that someone living in North East Lincolnshire can expect to fall into bad health eight years than the UK average, while the output of their work is also valued at £8 less than the average. The report argues that this is a vicious cycle and that factors like lack of job opportunities can harm people’s health.
To explore how good health can be the foundation for a fair and prosperous economy, IPPR is launching a new cross-party Health and Prosperity Commission. The cross-party commission will be chaired by Lord Ara Darzi and former Chief Medical Officer Dame Sally Davies.
The report argues that the UK’s poor health outcomes and stagnant economy are a result of poor policy choices. According to IPPR, policy makers must now ‘set about putting the building blocks of good health in place’, including ‘good work, quality housing, local public health services’ and a ‘well-funded and staffed NHS. ‘
Dame Sally Davies, former Chief Medical Officer and co-chair of the Commission on Health and Prosperity, said: “A fairer country is a healthier one, and a healthier country is a more prosperous one. While the restrictions have eased, the scars of the pandemic still remain deep on the nation’s health and our economy.
“Not only are we facing a severe cost of living crisis, driven in part by pandemic induced inflation, we’re also experiencing a workforce shortage driven by poor health that’s holding back the economy. It has never been more important to put good health at the heart of our society and economy – and our commission will bring forward a plan to do just that.”
Matthew Taylor, NHS Confederation chief executive and commission member said: “The pandemic has shown how deep health inequalities shape and cut across the lives and livelihoods of people across the country.
“Yet this is not new, disparities in health have not suddenly appeared, they have been part of the make-up of our society for decades. As millions of people now face the reality of a cost-of-living crisis there is an urgent need for a much bolder and more strident approach to tackling inequalities to create improved population health and stronger economic wellbeing.
“We are delighted to be part of the Commission on Health and Prosperity and look forward to reflecting member insight. ”
With the conflict in Ukraine raging, care employers are working together to provide opportunities for those displaced to work and find a home in the UK.
Care employers have been working together to understand how they can provide a meaningful employment opportunity for those displaced from Ukraine and other parts of the world and finding a home within the UK.
The National Care Forum (NCF), the leading association of not-for-profit care and support providers, in association with the Care Provider Alliance, have brought together a wide range of partners committed to offering support. This includes expertise from across national and local government, housing, recruitment specialists, legal and immigration experts and regulators.
Employers and partners are working closely with recruitment experts to enable displaced people from Ukraine and other parts of the globe to identify roles within the care sector, direct individuals to localised support and ensure that employers work together to provide the best opportunity for those who wish to work.
While this work progresses, the broader support for people displaced from Ukraine through the Homes for Ukrainians scheme is being clarified. Alongside this, local government has an important role in regards to how local support will work, and specific roles and responsibilities are still emerging. It is imperative that the desire to work is aligned with the need for displaced people to be connected into wider community and pastoral support.
Vic Rayner OBE, CEO of the NCF said: “Like many people affected by the plight of the people of Ukraine, care employers are pulling together to take action to help. The ideas are progressing at pace, and there is a strong desire to do something meaningful to help the people of Ukraine, and others from around the globe who arrive into the UK.
“We are pulling together opportunities for care and support employers to share details of available job vacancies, which we hope will be tied into the broader communications for displaced people. There are many other ways for people to offer support, including support to Ukrainians needing care and support, assistance with vetting and matching, and those who have a housing solution.
“However, there remain significant unanswered questions around regulatory requirements, right to work entitlement, safeguarding, etc. We need the government to work at pace alongside adult social care employers to resolve this. Furthermore, we are working with other partners, to understand how most effectively the sector can be engaged to provide a solution at this moment of crisis.”
More support needed for “fatigued” social care workforce
By Mary Brown
On the 16th March 2022, Public Policy Projects (PPP) hosted an evidence session entitled The Social Care Workforce: Averting a Crisis as part of its report series The Future of Social Care. PPP’s Social Care Network examines the most urgent issues facing social care and presents tangible solutions to address workforce challenges in the sector.
The crisis facing the social care sector is fundamentally a workforce one. The sector itself is a large employer in the UK, employing about 1.54 million people, equivalent to five per cent of the workforce. As one participant noted, “the sector itself is a huge contributor to the economy and to society”. Given that staff pay is the single biggest expenditure faced by care homes, workforce management should be front and centre whenever system finances are being considered.
Even before the pandemic, there were about 112,000 social care vacancies in England, with jobs paying only £8.50 an hour. Following the pandemic, the vacancy figures are assumed to be worse. Key issues driving individuals away from working in the social care sector include low pay, stressful working conditions and a low sense of worth.
A participant of the evidence session emphasised that the working conditions of the social care sector have led to 74 per cent of care professionals reporting that they regularly experience stress at work, an average number of sick days 25 per cent above the national average, and a staff turnover rate significantly higher than the national average.
As phrased by one participant, social care is suffering from a “fatigued workforce” not only due to the pressures of the pandemic, but issues which have existed within the sector for much longer. The problems within the social care workforce are chronic , and are considered by many to constitute a crisis. As one participant said, “clearly a workforce strategy is one of the absolute essentials that we need to have to make a success of the sector over the next decade or so”.
“The social care sector should work alongside recruitment organisations to recruit young, bright people into social care, and help them consider where a career may lead.”
One problem identified was narrow recruitment to the sector. It was stressed that within social care, “we should cast our nets wider in a recruitment approach… and recruit not only people with previous experience”. The social care sector should work alongside recruitment organisations to recruit young, bright people into social care, and help them consider where a career may lead.
It was also suggested that more effort must be made to recruit hard-to-reach and underemployed groups, including people living with disabilities, and immigrant workers. “What frustrates me is that there are individuals in these groups who can be wonderful, caring staff [but]are missed, because hiring managers are too narrow in their focus”, said one participant.
Staff retention rates in social care are low. Network members noted that social care workers often leave the sector for other, similarly paid jobs, such as retail roles, while few choose to leave and work for the NHS. One network member identified that “between care assistants in the NHS and the social care sector, there is around a 23 per cent deficit in social care. The terms and conditions are vastly better in the NHS. Pensions, sick pay, overtime and unsocial hours all contribute to that deficit.”
Essentially, social care workers are underpaid and undervalued. For both better recruitment and retention, social care workers must be appropriately paid and treated as though they are valued. Some network members identified low pay as the key driver for individuals choosing to leave the social care workforce, and yet, it was emphasised that social care is a both a skilled and psychologically demanding profession, and should be commensurately well-paid.
However, funding in the system is limited, and paying the workforce is the sector’s single biggest expense. One participant said “there is not a settlement from government or local government that actually meets the cost of care to enable us to pay a proper wage for the level of skill, ability, responsibility, dedication that [care workers] have”. Furthermore, a high proportion of social care workers are on zero-hours contracts; in London, this figure stands at 41 per cent of social care workers. Therefore, many social care workers have to deal with pay inconsistency and insecurity, on top of being low-paid.
“Network members were in agreement that social care is, and should be publicly regarded as, a skilled profession.”
While pay is regularly described as the most pressing issue in the workforce, one participant argued that in their experience of conducting exit interviews with workers, it is not low pay, but rather a low sense of worth which leads people to leave the profession. While higher pay is one way in which care workers can be practically appreciated, it was agreed that more must be done to value care work both by improving the public image of care workers and ensuring that internal structures provide support and give value to workers.
Network members were in agreement that social care is, and should be publicly regarded as, a skilled profession. “It is not the kind of job that everyone can do,” said one participant. “It is a skilled job, which requires the creation of quality human relationships and working with people who have complex care needs… it is a real skill and should be regarded as the same as working in health.”
Social work is challenging and worthy of respect, all participants agreed. One commented that “no two days in social care will be the same; you have to be agile and move with that, so it does take very special people to take those roles”. The public status of social care work must be elevated to reflect this, and the workforce to feel appropriately valued if these retention issues are to be effectively addressed.
Securing an integrated future
For a supported workforce, good leadership is essential. One participant noted that in the social care system “there is a varied approach to leadership”, and good leadership is not always evident in the system. Given the demanding nature of social care work, it is essential that carers feel well supported in their roles. One participant added that “workers do not stay because of a good job, they stay because of a good manager”, and therefore, proper leadership training must be a central goal of the workforce plan.
A practical solution suggested by one of the network members to combat low recruitment, retention and the poor image of the profession was a ‘social-care-first’ scheme, mirroring the successful teach-first scheme. Many other sectors have emulated the ‘teach-first’ template with great success. The aim of the scheme is to engage with young people to consider social care work as a career by espousing the value of a career in care. Such a scheme would emphasise how care work has the potential to transform the lives of dependent individuals, and the importance and value in building personal relationships with system users, improving the image of the profession. As part of the scheme, there should also be structured leadership, coaching and mentoring training, for the purpose of also transforming the quality of social care. This may serve to solve some of the leadership issues in the sector, as young and bright individuals will be well trained to manage and lead social care in the future.
Now that the NHS and social care are moving towards integration, participants noted that for a true and fair integration of the systems, employees should be paid and treated equally. One participant called for a joint recruitment scheme for the NHS and social care, with equal pay offered. It was also emphasised that NHS workers receive many ‘perks’, particularly since the start of the pandemic, which social care workers do not (including food and drinks discounts from certain companies).
Other suggestions to aid the integration of the NHS and social care workforce included social care placements and secondments for NHS staff, in which they are exposed to social care, and the richness and value of social care work. The status of care work must be elevated for proper integration of the two systems can occur, in order that social work and NHS work can be equally respected.
A large part of the discussion focused on the role of volunteers within the social care sector, and the value they bring to both paid carers and system users. Volunteers are an invaluable part of the social care workforce given that they reduce pressure on care workers, improve patient experiences, facilitate higher quality of care to drive better health outcomes, and strengthen community connections. One participant said that in the context of social care, “volunteering is a public health tool. There is a body of medical research which talks about the huge benefits for mental health and physical wellbeing for patients”. Volunteers also serve to raise the visibility of the social care sector.
Since the start of the Covid-19 pandemic, the UK has seen an unprecedented rise in the numbers of people volunteering in their local communities. During the pandemic, the UK had 12.4 million people volunteering in their local communities. 4.6 million of these were first-time volunteers. Currently, the UK has a window of opportunity to make the most of the interest in volunteering to reduce the immense pressure on care workers.
As part of the workforce strategy, there needs to be investment to drive the volunteer sector, for the wellbeing of the social care system and its users. However, time is undoubtedly of the essence; as one participant emphasised, “there is an urgency to the conversation we are having. As Covid dissipates, what we don’t want is for people to go back into the corners of their community and not come out again to contribute.”
Digital Health Academy to provide free digital skills training
By Gabriel Blaazer
The Digital Health Academy opens today and aims to provide free digital skills training to all NHS staff by 2031.
From today, the Digital Health Academy, a free, digital training tool for NHS frontline staff, is in operation. Aimed at providing digital skills training to all NHS staff by 2031, the modules are now freely available on the Health Education England NHS Learning Hub. As highlighted by Health and Social Care Secretary, Sajid Javid, in a recent speech, it’s crucial that the NHS improves digital provision across all health and care services and the Digital Health Academy aims to address this by building on the digital skills of all NHS staff.
A survey from the Organisation for the Review of Care and Health Apps (ORCHA), reveals that although 65 per cent of the public are open to trying digital health technologies, only a fraction of tools are recommended by health or care professionals.
In total, amongst those using digital health, only a small proportion of recommendations came from healthcare professionals, with 17 per cent of recommendations coming from GPs, eight per cent from hospital doctors, and two per cent from nurses.
The need to support a digitally ready workforce has been highlighted by the NHSX Readiness Plan and the CPD-accredited Digital Health Academy responds to the critical requirement to invest in developing front-line skills for digital health through professional development.
Currently, there is still no mandatory digital health training for health and care professionals, and the courses that frontline workers can attend are often scarcely available. In response to this need, ORCHA, with the support of universities and healthcare professionals, and with financial support from Boehringer Ingelheim, developed the Digital Health Academy, the foundation level modules of which will be freely available at orcha-academy.com and on the Health Education England NHS Learning Hub.
The academy’s online training modules are designed specifically for frontline health and care professionals who want to use and recommend digital health tools but have been struggling to access the knowledge to do so safely.
ORCHA has created the infrastructure of the online training portal and designed courses, drawing on experience gained reviewing more than 17,000 health apps and operating health app libraries in 70 per cent of NHS regions.
The Digital Health Academy’s aims include:
Free access for all NHS and social care staff
Availability on Health Education England NHS Learning Hub
Enabling staff to gain Continuing Professional Development (CPD) points in a vital new area of professional development
The CPD-accredited Digital Health Academy programme includes:
Short, bite-sized learning modules to suit busy schedules, which can be accessed at any time
Two foundation modules which explain the function of health apps, the current digital health landscape, the barriers to using and adopting digital health and the importance of prescribing good quality digital health products
Coming soon, a series of specialist modules including topics such as digital health for mental health, diabetes, physiotherapy, long Covid and winter pressures
Commenting on the academy’s resources, Dr Neil Ralph, Head of Health Education England Technology Enhanced Learning (who has previously written about the need to prepare the NHS for digitally-driven healthcare), said: “COVID-19 accelerated the rapid adoption of digital health across health and care services and the need to embed digital health in the long term. We are delighted that ORCHA has contributed its Digital Health Academy foundation content to the Learning Hub and look forward to hosting new content in the future, further supporting health and care professionals in their roles.”
Learning about the value the Academy offers frontline staff, Boehringer Ingelheim committed to sponsor the foundation modules. This has enabled it to be opened up at no cost to health and care professionals. Commenting on this, Uday Bose, Managing Director at Boehringer Ingelheim UK & Ireland, said: “There’s widespread recognition of the need for digital health training for frontline workers, with organisations from the King’s Fund to the Royal College of General Practitioners calling for it. With six million people now waiting for elective care, and with first-class digital tools available which could support healthcare workers with many of the high volume and low complexity cases, the need to improve digital skills and digital confidence in the NHS has become critical. We felt the academy was a perfect way to address this very real need amongst frontline staff.”
Ahead of the launch, the academy has been introduced to professionals using the ORCHA digital health libraries to a positive reception:
Dr Michelle Webster, Chief Clinical Information Officer & Consultant Clinical Psychologist at Coventry and Warwickshire NHS Partnership Trust, said: “The ORCHA Digital Health Academy has helped to demystify digital health, strengthen our clinicians’ digital skills and boost their confidence in using healthcare apps. The bite-sized modules are easy to follow, interesting and relevant and designed to flexibly fit around their busy jobs. I would highly recommend.”
Najia Qureshi, Director of Education and Professional Practice, British Dietetic Association, said: “This is a really welcome resource for our members, who work across the NHS supporting patients with a wide range of health conditions. Innovation in healthcare is introducing new ways of working and is transforming patient care. This programme will help dietitians and other health and care professionals to develop the professional skills needed to confidently use and recommend the right digital health products – helping patients to benefit from digital healthcare.”
Reviewing a foundation module course, Dr Joel Brown said: “It takes quite a paradigm shift to move physicians away from seeing prescribing as an exclusively pharmaceutical enterprise. As medicine is increasingly digitised, clinicians need to take seriously the opportunity to prescribe digital health. The course by ORCHA, as part of their Digital Health Academy, makes this point brilliantly.”
Taking practical steps to address a growing crisis in domiciliary care
By Gabriel Blaazer
John Bryant, Head of Strategy and Development for Torbay Council, outlines a series of practical steps to enhance the role of the care worker and address the growing crisis in domiciliary care.
The solution to the domiciliary care crisis is to enable the sector to do more, not to simply ask more of it. The distinction is important, as the development of integrated care provides opportunities to enhance system efficiency like never before. And yet, the scope of what could be asked of, and performed by, trained, supported, committed community-based practitioners is yet to be fully explored or achieved.
All the while, the expectations of those receiving care, and certainly those considering a future career in health and care, are greater than they have ever been.
To meet these ever-rising expectations, system leaders are likely to find fertile ground in looking to better embrace the assets that already exist within the system. This includes domiciliary care workers, whose skillset could be expanded and developed, a move that could encourage others into the system. This can happen by re-positioning the expectation, skills and rewards to produce and provide, for example, enhanced wellbeing services (EWS) provided by enhanced wellbeing practitioners (EWP), of which domiciliary care is a major component among a portfolio of beneficial interventions and service provision.
The 6Cs of care are prevalent within our frontline domiciliary partner staff; the opportunity is there to optimise their engagement and knowledge of patients and clients to:
Support retention and recruitment
Respond to the discharge and reablement challenges
Drive early intervention and prevention
Offer a developed interface with general practice
Engage with population health management
The support of these four key drivers for public service change: politics, policy, measurement and money, are positioning us as never before to achieve success. The government’s social care reform white paper, People at the Heart of Care, connects to the £5.4 billion pledged for adult social care reform between 2022 to 2025. It is notable that healthcare is a major beneficiary of this funding in early years, however within the policy of integrated care the opportunity exists to bring about radical, beneficial system reform from the outset.
“Together, these measures aim to put people at the heart of social care and move us towards our 10-year reform vision.”
(Department of Health and Social Care, 2022).
These themes were also present in the subsequent integration white paper, Joining up Care for People, Places and Populations. The measures set out in the paper provide clear areas of opportunity, focus and policy support.
A growing crisis
These government white papers are in no small part a response to a care crisis the likes of which we have never seen. One key element of that is domiciliary care, the unseen service that is delivered behind the front doors of our communities to keep people safe, comfortable, medicated and cared-for. For over a decade the policy has been to bring care closer to home, and the People at the Heart of Care paper reinforces that. The Covid-19 pandemic has compounded the need to ensure people are cared for and supported in this way, minimising their movement between different health settings to reduce infection risk.
“The endeavours of care providers to recruit at this level should be celebrated alonside any other part of the system that has been able to do the same”
Present estimates indicate that there is a care shortage/vacancy rate of 17 per cent which equates to at least 100,000 jobs based on Skills for Care data in England. Given the challenges in recruitment felt by providers, there can often be a projection that care providers are not ’good‘ at recruitment. However, in looking behind the headlines we find that in one area, Torbay, care providers have increased their capacity through recruitment by 39 per cent in the 18 months leading to September 2021. The problem is that the demand for their services has totally outstripped this staffing influx, increasing by 47 per cent in the same time period. This trend is consistent across the country’s health and care ecosystem.
The endeavours of care providers to recruit at this level should be celebrated alongside any other part of the system that has been able to do the same. If organisations who have been able to recruit as well as Torbay have done are finding it difficult, is it probable that any other part of the system will do better?
The Health Foundation recently published research suggesting that over a million more health and care staff will be needed in the next decade to meet growing demand for care. What is clear is that these shortages were well established trends before the Covid-19 pandemic. If the challenge of capacity is to be permanently addressed, then retention followed by recruitment is essential – as any marketing of roles from ‘the system’ will be trumped by the messages communicated by those working in or leaving the services.
Recognising a new future, communicating that and providing examples of what could be achieved will produce opportunities for beneficial results.
Practical steps
In this respect, returning to the domiciliary care issue, what might emerge if we were to turn the issue on its head?
To address the crisis currently seen in domiciliary care, I propose a series of practical steps to enhance the role of the care worker and to use the ICS framework to transform system level efficiency:
Addressing the domiciliary care shortage: expand the potential of the service and provide those delivering it with more responsibility and control by becoming EWPs
Supporting the community nursing challenge: offer them the opportunity to have a wider team of EWPs at their disposal; enable them to work to the top of their licence
To address GP availability: create neighbourhood teams of EWPs that are able to be with patients, directly support with digital literacy and connectivity, and be a physical presence to further enhance the experience of the remote general practice
To reduce A&E admissions and improve the discharge process: use EWS to support the safe discharge of increasingly complex patients to optimise recuperation in at-home settings, have the digital skills and tools to monitor and report e.g. RESTORE2 for early intervention and re-admission avoidance, and be able to support reablement; the stepping stone to independence
Develop greener care:reducing mileage by minimising cross-overs between staff and building a wider multi-disciplinary team
The practical possibilities for this are supported by the further development of the Allied Health Professionals strategy. The publication of the Allied Health Professions’ Support Worker Competency, Education and Career Development Framework received support from Trades Unions, Professional Bodies and Trade Union partners. Whether it is development within roles or providing new career paths, new forms of offer and opportunities are going to be central in encouraging a post-Brexit, domestic workforce into the social care and health sector; along with producing the impact value of those roles and associated care interventions which enable commensurate levels of pay and reward.
Underpinning all endeavours and quality care and support are the 6Cs of Care. These emerged as part of ‘Compassion in Practice’ and were rolled out by NHS England to all staff in 2014 with subsequent promotion to the wider care sector by the national body Skills for Care.
“But what cannot happen is that domiciliary care continues to be overprescribed without receiving more support or being allowed to expand its offering”
The characteristics of commitment, care, compassion, competence, communication and courage are prevalent throughout our community care partners and their staff. With that commonality between the professions what might we do to deliver even more fulfilling roles: more people doing fulfilling roles, more fulfilment within the roles, more roles in addition to the present ones that are also fulfilling?
The alchemy that will bring this about is within the gift of every system in England and available to all domestic nations. It is the meaningful flourishing and delivery of an integrated care system (ICS). The ‘holy grail’ of ICS development is to provide timely, personalised care that maximises the independence of the individual receiving care which, naturally, points to a home-based solution. But what cannot happen is that domiciliary care continues to be overprescribed without receiving more support or being allowed to expand its offering.
This article seeks only to look at one small area of that; however, it is a vital area, being felt by the 957,000 people in the UK that receive domiciliary care and their families, along with the 822,000 staff looking after them (as recorded by RCN surveys). This, quite rightly, is now receiving both political support and national media attention.
The pandemic should be recognised as a catalyst for accelerated change, avoiding any sense of ‘once we’re through this we can get down to business as usual’. What has been done, and is being done in response to the pandemic, has demonstrated the creativity and pace of change possible as system partners have collaborated. Fostering and building on that is in itself both an opportunity and a challenge.
Across the sector there are understandable concerns of implementing radical service reform on an already exhausted and beleaguered workforce. But there are examples we can look to where workforce wellbeing is protected while simultaneously enhancing capacity and quality of care that motivates staff.
Some facts from one system
To service 800 clients in a 75-mile geographical perimeter, home care staff drive almost one million miles per annum. In work supported by the Health Foundation, it was found that at a (sub)urban travel speed averaging 20 mph, over 43,500 hours were being spent in vehicles; a substantial proportion of that could be put to new ways of working.
Work has shown that by reorganising the rounds, 5,220 hours of care could be released from the existing workforce. This would provide opportunities not only for more care to be delivered but importantly, and in respect of future retention and recruitment across the system, time for wellbeing, supervision, learning and development, accreditation of skills and assurance in their application. And with no extra hours of care being purchased.
In terms of application and the development of broader multi-disciplinary teams within ICSs, it was established that of the community nursing patients nearly 20 per cent were also social care clients. People were being visited by multiple staff in one day, requiring travel from multiple staff.
There are of course many activities and health interventions which can only be done by those with nursing and clinical qualifications. However, in approaching this issue with a mindset of curiosity, courage and compassion there are many interventions that could be performed in different ways.
For instance, one of the many activities that domiciliary care staff undertake is washing and creaming clients’ legs when there are wounds to be attended to. Nursing staff will then arrive to apply a bandage. While certain grades of wound clearly need nursing attention there are many at lower levels of severity that are capable of being attended to by a well-trained EWP – and of being checked on regularly, though less frequently, by the stretched community nursing complement.
Benefits of EWS for participants and for system development
Enhanced wellbeing practitioners:
Feel respected and able to develop their domiciliary care roles, feel even more a part of the system and that their contribution is valued. This could lead to enhanced profile and esteem. The additional activity means more time with the client and the opportunity to further enhance the relationship that exists
Opportunities will be presented to work in strengths-based ways and with programmes such as Making Every Contact Count, leading to enhanced wellbeing of the clients and a development of their connectivity and circle of support
This leads to improved job/role satisfaction – improved retention leading to increased recruitment. Developed circle of support for clients, enabling them to step up towards independence and reduce their reliance on statutory interventions. Release of capacity for those with assessed needs to have their needs met and begin their journey towards well-being
Community nurses
Feel an increased level of support with a bigger, more integrated, team available to them. They are then able to work with the more complex cases and make the very best use of their skills and knowledge while enabling and supporting other integrated team members to develop
Through enabling better management of case-loads, job satisfaction is increased and stress is reduced. As the RCN has established, with 75 per cent of community nurses reporting that they had left necessary activities undone, the professional dissonance of the role is alleviated, supporting staffwellbeing and retention
With the nursing and Allied Health Professional colleagues active in this way, early intervention and reductions in exacerbations of conditions lead to reduced admissions. With greater capacity, along with the skills to manage more complex discharges, hospital flow is improved
Benefits of EWS for health providers
Admissions through A&E:
Are reduced by earlier interventions and the ability to deploy the highly skilled staff in the community to support patients and reduce the deterioration in their condition
Improved flow through A&E with reduced admissions, enhancing the wellbeing of staff as well as the patients, and contributing to the enhanced application of funding to meet elective care
Discharges and re-admission rates:
Are further improved with the skills and capacity made available to support increasing numbers of and increasingly complex patients. With the integrated approach to working and early intervention opportunities, people are supported to remain at home, with their condition even better managed and do not require a re-admission to hospital
Skills and capacity across the community integrated team are available to support timely, safe discharge from hospital and discharge to assess and ensure people remain at home
The patient/client gets less ill and recovers more quickly being supported by a team that has the resources, capacity and skills to meet their needs. This increases the ability for them to remain well or recover quickly in their home setting, which include care homes and supported living
Increased numbers of people cared for closer to home with reduced exacerbations in conditions. Complex clinical requirements being met in community settings with both care-giver and the patient having a well developed strengths-based relationship throughout the care and support period, enabling a step up to independence
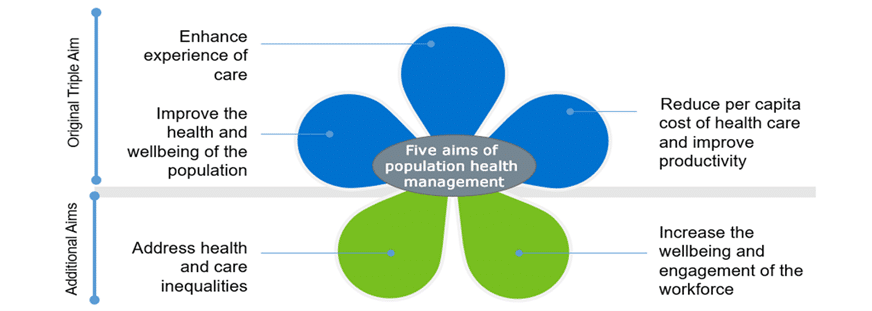
It is understandable that there will be anxieties associated with the shift in activities. In order to ascertain who delivers what and where to achieve the five aims of population health management (as illustrated below), the mantra to hold onto is right person, right care, right place, right time. Risk-managed prototyping using good design methodologies is key and implicit within the title on the tin of sustainability and transformation partnerships (the predecessor to ICSs).
There are many practical examples already available and still plenty of headroom for further development, which will accelerate the transformation in health and care models which are both sought for and needed.
Covid has shown us how much can be done in a short space of time; even with all the pressures in the system, GPs, acute trusts, AHSN and domiciliary care providers worked together to train 148 staff in the RESTORE2 methodology in just three months, with some going further to be trainers themselves.
Practical steps to developing and implementing enhanced wellbeing services
Train domiciliary care and care home staff to use the protocols and develop relationships with primary care practices
Ensure that training is accessible and that the nursing staff are corporately supported in the delegation of tasks
Look to see if care packages are allocated by geographically focussed provider or on first-come-first-served basis, and what the mileage component to the care rounds is for providers
Review the wounds being attended to in community settings and what best practice can offer in tackling the £5 billion cost of wound management
Consult on ways in which the Allied Health Professions’ Support Worker Competency, Education, and Career Development Framework can be optimised
Get the best facilitators and design thinkers, often found outside the system, to help ask the questions, listen and gather the answers and develop action-orientated plans with system partners – which includes the care unit, the patient/client and those caring for them
Whichever of the four policy drivers (politics, policy, money or measurements) one wishes to consider, they are captured within the Five Aims of Population Health Management; moving to EWS and development of the practitioners supports their delivery. Beyond this the one element that is maybe more implicit within the ‘petals’ below is capacity. EWS supports this explicitly.
Achieving more with less
In summary, below is the 30-second elevator review of how we can achieve more with less on the topic of domiciliary care.
More:
Time to care, more time to be more caring
Development and enrichment of roles
Person-centred care
Satisfaction with the role
Retention
Recruitment
Prevention and early intervention
Less:
Dissonance in the role and 6Cs
Siloed working
Variation in care team and discontinuity of care
Dissatisfaction with roles and system design
Turnover and leaving before retirement, or at the earliest opportunity
Vacancy and cost to trying to encourage people into services
Illness and cost
Addressing the care crisis
With the job-seeking public indicating that insufficient numbers of them wish to work in domiciliary care, now would be the time, supported by the policy of integrated care, to develop a new offer that enables truly integrated roles. This should seek to provide enhanced wellbeing services through an increasingly broad, multi-disciplinary, person-centred team.
To address this multifaceted care crisis, we should do more than seeking to invite people into traditional domiciliary care. The system might benefit from offering people a new role(s) that encompasses the domiciliary care that they are proud to already be doing, but also one that offers development, inclusion, satisfaction, esteem and commensurate compensation. This could become increasingly available if and when ICSs fulfil the potential that exists; one that reflects those stated aims within the recent white paper(s) and meets the five tenets of Population Health Management.
This should also note the observations of the CQC and their likely support to engage in discovery sessions for regulation alignment towards new ways of working. In doing so this should create a virtuous cycle towards a sustainable system, both financially and with capacity, through the delivery of integrated care.
John Bryant is Head of Strategy and Development for Torbay Council and an ICJ contributor. To contact John, become an ICJ contributor or to obtain a full reference list for this article, please write to news@integratedcarejournal.co.uk, and one of our Editors will assist.
To achieve the NHS Long Term Plan goal of preventing health inequalities and improving health outcomes, the voices of those delivering and receiving dental care on a local level must be prioritised.
Top-down change, if not informed by local experience, will fail to address issues faced by service users and service providers. Therefore, the voice and experience of local councils, local Healthwatch and local service providers is key to creating an environment through which NHS dentistry can play its part in reducing health inequalities and improving health outcomes. This is why building strong relationships with these bodies is central to the role played by Local Dental Committees (LCCs).
The LDC Confederation is a membership body for LDCs which represent primary care dentists delivering care under an NHS contract. We actively support our member LDCs to engage with local stakeholders, to take the time to explain the complex NHS dental contract and to make clear how, if properly supported, NHS dentistry could help meet their local objectives. These local relationships have created sympathetic alliances and a strong desire at the local level to see a reformed dental contract introduced that would remove barriers to care, which in turn would help to reduce health inequalities and improve health outcomes.
The local councils and local Healthwatch know their populations, understand their issues and seek to identify areas for improvement. Even before the pandemic, we were pleased to see a growing interest in NHS dental services from local stakeholders. Since then, of course, we have seen access to NHS dental services and appropriate provision of NHS dental care grow into a burning issue for almost every local authority.
Member LDCs have enjoyed close working with their local Healthwatch partners, helping with reports and speaking at events throughout London. During the pandemic we provided updates and patient facing information for our local partners to help them and their communities to navigate NHS dental services. This interest has increased dramatically throughout the pandemic as services have struggled to meet patient demand.
Barriers to access
The barriers to access exacerbated by the pandemic have existed since 2006. The pandemic simply brought them to the fore and demonstrated the historic neglect that NHS dentistry has suffered, but also the huge importance that the public place on NHS dentistry. Time and again we have seen reports which show clearly that dental services are highly valued and that satisfaction with the quality and outcome of the care received is high.
NHS dentistry should be one of the great success stories within the wider NHS: a high achieving clinical specialty, with high patient satisfaction, providing clinical care able to give instant pain relief and rapid functional outcomes. Instead, sadly, it is treated as an ancillary service which is not vital to health and wellbeing.
Local stakeholders know differently. They hear stories from patients in pain on a regular basis, from parents of children in pain, from those who are ashamed to go out or eat in public, from people who are afraid to access care because of the NHS charges and those who simply cannot navigate the system and end up at the GP or in A&E. We have been working hard with local partners to press for improvements to holistic care, especially for the most vulnerable such as those in residential care homes and those with conditions such as Alzheimer’s and other dementias, diabetes and stroke rehabilitation. These groups in particular need the system to work with them and for them if they are to lead lives free from avoidable pain and discomfort. Integration of services at the local level will support a holistic approach to care which would pay dividends in improved general health outcomes and quality of life.
Dental contract pilots
Dental contract pilots, later termed prototypes, have been the great hope of the profession since they began in 2010. These pilots were testing new models for the contracting of NHS dental care and were based on blends of capitation and activity. Appointments were longer and the focus was on prevention.
90 per cent of patients had reduced or maintained levels of tooth decay
80 per cent of patients had reduced or maintained levels of gum disease
97 per cent of patients said they were satisfied with the dental care they received
At the start of 2022 the NHS announced the end of the prototypes and all dental practices operating as prototypes for the NHS are now reverting to their previous contracts. Despite the models showing such promise it is not clear how much of the valuable information taken from these pilots will be applied to a reformed contract in the future.
Local voices are vital
The current Units of Dental Activity (UDA) contract, is based on activity and the NHS is heavily reliant on recouping funding for dentistry through patient charges. This creates a disincentive for the system to increase access among those with the highest need, as a greater number of treatments take longer and in doing so will reduce the amount of activity delivered, throughput of patients and the amount of funding the NHS can recoup from patient charges. The current activity based contract is not able to support local objectives of reducing health inequalities, and the focus on treatment rather than prevention does not support the local objective of improving health outcomes.
If the local councils, and in the future local care partnerships and Integrated Care Boards, want to see a reduction in health inequalities and improvement in health outcomes then a dental contract which supports those objectives is needed. The LDC Confederation ensures that local stakeholders understand NHS dental services and the role they can play in meeting these priorities. We will continue to work with our local partners to make sure local voices who know their populations best will be heard at the national level. Local voices are vital to inform dental contract reform and to make sure that the dental contract is fit for purpose.
The Minister for Primary Care, Maria Caulfield, recently outlined the aforementioned problems with the dental contract on BBC Radio Sussex, and also affirmed the importance of contract reform. Both of these statements are to be welcomed but real improvements will only be seen if that reform is based on the experiences and priorities of those delivering and receiving care at the local level.
Is the answer to improved health hiding in plain sight?
By Dr Anne Elliott and Professor Tim Evans
The UK is suffering from a major gap in the provision for exercise as a prevention or management tool for chronic disease. Outlining this growing healthcare crisis is Dr Anne Eliott, Senior Lecturer in Physical Activity for Special Populations and Healthy Ageing, and Prof Tim Evans, Professor in Business and Political Economy at Middlesex University London.
Over and above record NHS waiting lists1 and the adverse effects of the Covid pandemic, there is a tsunami of chronic disease on the horizon, and it is flowing towards us at a stately and predictable rate2. We can see the wave growing and developing, we can gauge its potential cost, we can foresee the amount and quality of resources that will be needed, and we can estimate the number of specialist healthcare professionals that will be required to address it – and yet we seem unable to avert what increasingly appears to be an inevitable disaster.
We cannot lay the blame for the growth in long-term illness on a lack of health education, as positive health messaging from both the state and private sectors is prevalent in all popular media and easily accessible for all age groups and populations. At the bare minimum, the general public understands the importance of ‘eat less’ and ‘move more’. Over the last 20 years, successive governments have sponsored numerous initiatives that have attempted to address such issues, from Change4Life (PHE 2009) that aimed to encourage families to exercise together, to the recent adoption of an old idea, social prescribing3 (NHS 2020), that targets loneliness and depression at a local community level.
However, differing socio-economic determinants have been identified as obstacles to participation. Although authorities try to address these barriers, sedentary behaviours and lifestyles are responsible for 40 per cent of premature mortalities and continue to be the weak spot for ‘preventative medicine’4, a term now well established within Parliament and across the UK’s broader political discourse.
Cost is consistently found to be one of the biggest barriers to moving towards a healthier lifestyle. Through physical activity in the private sector and with levels of economic status found to be correlated to health outcomes5, it would be beneficial to make access to exercise easy as both a preventative tool in the public sector and as a response to the onset of many diseases further adversely impacting the medical sector.
A gap in provision
There is a clear gap in provision for exercise as a prevention or management tool for chronic disease and there isn’t availability or knowledge in the existing medical workforce to bridge it
At present, general practitioners are the most efficient and effective pathway to intervention and support for people in local communities. However, there are limited options, such as exercise referral schemes6, found to be too short for exercise adherence and too expensive for most practices to utilise, or referral to a scheme such as the NHS Diabetes Prevention Programme. Apart from these ‘schemes’ the next level of physical specialism is physiotherapy and associated disciplines which are geared to address more clinically acute rehabilitative issues.
It is against this backdrop that there is a clear gap in provision for exercise as a prevention or management tool for chronic disease and there isn’t availability or knowledge in the existing medical workforce to bridge it. However, with some creative change and investment, the workforce required to fill this gap could be closer at hand than most commentators realise.
Currently, there are approximately 66,300 fitness instructors in the UK, of which 22,032 are personal trainers. They are well placed to work with the general public with diagnosed or undiagnosed chronic conditions – it is common for sufferers to live with low level conditions for up to 20 years before they seek help from their doctor, when the condition interferes with their quality of life. The Chartered Institute for the Management of Sport and Physical Activity (CIMPSA), acknowledges this specialist need and has drawn up professional standards for fitness7. Ukactive8 also discussed using trainers more within a wider community based social prescribing framework. We see professional bodies turning their consideration to this in light of Covid, which has created an awakening of understanding for the need to improve the physical and mental health of an ailing population.
Upskilling the workforce
While such upskilling requires investment, the costs will not be as great as leaving health outcomes to an unnecessarily disjointed and unreformed skills base
The fitness workforce has historically been eschewed by the medical profession on the basis that too many of its practitioners lack appropriate levels of educational attainment. Personal trainers are shown to have qualifications that range from a ‘two-week online course’ to a Masters degree in a sport specialisation such as Strength and Conditioning. Industry regulation has mitigated this to a certain extent by registering most practitioners with a vocational qualification equivalent to an A level. However, these fitness qualifications are not mapped to any NHS accreditation and qualification requirements and so a divide between health provisions runs deep.
An obvious solution to this division is to bring existing fitness qualifications into parity with the medical regulatory framework. The workforce can be upskilled into the range of existing NHS levels of qualifications and pathways, such as apprenticeships, which may then provide an opportunity to create roles acknowledged by the Health and Care Professions Council.
While such upskilling requires investment, the costs will not be as great as leaving health outcomes to an unnecessarily disjointed and unreformed skills base. At a time when the NHS is facing its largest ever backlog, it would be wholly inappropriate to invent a new category of worker, train them from scratch, or alternatively do absolutely nothing.
Workforce planning
While in the past the pressures of electoral politics have often prohibited effective workforce planning, inaction with regards to the country’s fitness workforce is contributing to a multifacted healthcare crisis
To mitigate the ill effects of both the waiting list backlog and the coming tsunami of chronic disease outcomes, it is important to make key investment and workforce planning decisions now. These plans should ideally be locked into our health system for the longer term through a robust cross-party agreement.
For decades, successive British governments of all stripes have avoided workforce planning issues. Incentivised by shorter-term electoral cycles, they have instead left the healthcare system dangerously exposed to the fragilities of professional overstretch. This is why the UK has so few doctors and nurses in comparison to other comparable countries in the developed world9.
However, with today’s spiralling costs, waiting lists setting ever higher records and more than 21 per cent of people now opting to use private healthcare10, the NHS urgently needs creative solutions if it is going to have space to develop and implement better planning.
It is in this context that this proposal to upskill and realign existing professional skills and resources makes so much sense. As a swift and effective solution to overcome a current and costly chasm in our health system, the objective has to be not only holding back the looming wave of chronic disease but to enact comparatively inexpensive reform that will mitigate its most damaging and costly effects.
Faced with an unprecedented and systemic crisis of demand, the time for imaginative supply side reform is now more pressing than ever. If several tens of thousands of people are not empowered to fill the gap in our health economy, then the NHS – and the electoral support that it has hitherto enjoyed – could become irreparably damaged. While in the past the pressures of electoral politics have often prohibited effective workforce planning, inaction with regards to the country’s fitness workforce is contributing to a multifacted healthcare crisis.
Mind the Cap: choices & consequences for financing social care
By Francesco Tamilia
The government has announced its plans for social care reforms – but do they go far enough to address the issues endemic to social care?
Reforming social care – particularly with regards to financing it – has been a major challenge for successive governments over the past decades. Despite widespread acknowledgment of the need to reform the system, it remains in flux. In 2019, Prime Minister Boris Johnson pledged in his maiden speech that he was going to “fix social care”. Following the Covid-19 pandemic, the government has put forward clear proposals for reform – including addressing financing issues by increasing National Insurance contributions by 1.25 per cent to establish a new ‘Health and Social Care Levy’.
To discuss the financing challenges in social care, Public Policy Projects (PPP) hosted a roundtable with senior stakeholders in the sector as part of its “The Future of Social Care” report series in January 2022.
Lack of funding a chronic issue
The new social care reforms were broadly welcomed by participants, although many also expressed concern that the reforms do not go far enough to comprehensively address the depth of the issues in the sector.
“We simply don’t spend enough money on it.”
Lack of funding was, by far, the most recurrent theme of the discussion, with one attendee citing lack of adequate funding as the root cause of current market distortions in the first place.
He argued that “we simply don’t spend enough money on it. Every year, the Budget comes around, and when the social care system continues to be completely on its knees, the Treasury simply adds an extra billion pounds. This is immature. If we have to put an extra billion pounds into social care every year, then let’s say ‘over the next five years, we are going to put an extra billion pounds every year into social care’ so that care providers can plan. And then we don’t have the ludicrous chaos that we have at the moment, there is a barrier to planning there. We have to spend more on social care – and this is not just about older people, it’s about working-age adults as well.”
Where’s the money?
Speaking on the same issue, another attendee referenced historical funding in the care sector and highlighted how insufficient funding has led to an unsustainable market. He illustrated how social care expenditure over the last decade has increased since 2015-16, peaking at record levels in 2021 – largely due to the extra money that went into the system due to Covid-19. Roughly half of spending is on working-age adults and the other half is on older people. Money is indeed coming into the sector, but the question is: where exactly has the money been spent, and is it anywhere close to what is needed?
“The money coming into the system has not been spent on improving access and bringing more people into the system/”
Addressing the first question, the same attendee said, “the money coming into the system has not been spent on improving access and bringing more people into the system.” Consequently, eligibility for care has continued to tighten and has not risen in line with inflation, thereby excluding more people from the publicly funded system.
If that money hasn’t gone on improving access for more people, where has it gone? The answer seems to be on the average fees that local authorities pay for care homes. Indeed, there has been, in real terms, a 4 per cent increase in what local authorities pay for working-age adults and a 17 per cent increase in what they pay for older people’s care. “I don’t think you could argue that the extra money has gone on improvements in quality. Quality measures have stayed static over this period and Care Quality Commission (CQC) ratings have nudged up. Satisfaction ratings of publicly funded clients have also stayed pretty much the same. It seems much more likely that [the extra money] is going to fund home care and care home fees,” the same participant added.
Risk pooling a welcome step
“The private sector will never provide pooling of this catastrophic risk.”
A move by the government that was particularly welcomed by attendees was the notion of risk pooling social insurance. Rather than facing a potentially very uncertain risk profile, everybody effectively pays the same amount and is then covered against those risks. “That is undoubtedly what we should do.” said one attendee. “Social care is the only big risk that we all face where neither the state nor the private sector provides risk pooling. The private sector will never provide pooling of this catastrophic risk, it must be done by the state.” According to him, taking away the catastrophic risks gives us a chance of getting a market that will work not just for individuals, but for providers as well.
Overall, there was widespread agreement that although the new proposed legislation is a step in the right direction, more needs to be done to properly address the chronic financing issues in the sector. Yet, it’s equally important that any money that comes into the system is allocated wisely. Achieve this, and the many other issues in the care sector such as workforce and market fragility, can then be addressed.
This write-up forms one part of the wider Public Policy Projects Social Care Policy Programme. Drawing together key stakeholders from across the private sector, PPP intends to lead the debate on social care reform, to scrutinise and discuss the Government’s plans as they are delivered. Led by the Rt Hon Damien Green, the network continues to convene regularly for high-level strategic roundtable discussions in order to gather intelligence, insight and experience to deliver its recommendations through the publication of four reports.
1. Integrating Health & Social Care: A National Care Service
2. Mind the Cap: choices & consequences for financing social care
3. The Social Care Workforce: Averting a Crisis
4. A Care System for the Future: Digital Opportunities and the Arrival of Caretech
If you are interested in learning more about this significant programme of work, get involved in our work and partner with Public Policy Projects, please reach out to carl.hogkinson@publicpolicyprojects.com
Vaccination as a Condition of Deployment: When will the Government listen to social care providers?
By Louis Holmes
On 31 January, Sajid Javid, Health and Social Care Secretary, announced a U-turn on the Government’s Vaccination as a Condition of Deployment in health and social care settings (VCOD) policy. This move was anticipated by the press but for providers evoked despair and frustration.
VCOD 1 came into force on 11 November in the care home sector, and its impact cannot be understated. Since the passing of the regulations on 22 July 2021, it has been estimated that up to 40,000 workers have left the sector, a much larger sum than the estimated 12,000 which Mr Javid noted in his statement to Parliament. Since the statement, this figure has been withdrawn, but it demonstrates the Government’s contempt for the sector and lack of understanding of the impact VCOD has had on providers.
As England’s largest and most diverse representative body for independent providers of adult social care, Care England has been at the forefront of the VCOD discussion. The organisation has responded to the consultations for VCOD 1 and 2, along with advising the Department of Health and Social Care (DSHC) on what the Government must do to ensure the sector’s sustainability.
The VCOD timeline:
On 20 January 2022, the Department of Health and Social Care (DHSC) published the guidance for VCOD in wider social care settings.
Seven days later, on 27 January 2022, DHSC held a webinar for care providers, where the guidance was discussed, along with the Care Quality Commission’s (CQC’s) approach to inspections under the new regulations. DHSC even noted that further guidance was expected to come in the following days.
As As required by the implementation of VCOD on 1 April, the care sector was putting in the correct measures to comply with the new regulations, only to discover it was all in vain.
Equal partners
Although there are numerous contributing factors to a decrease in the workforce, it cannot be denied that VCOD was a significant reason. When the adult social care workforce was on its knees, VCOD dealt another blow. Since 11 November, there have been continued reports of care home closures, and throughout Christmas, there were serious concerns about the sector’s sustainability. But providers and their staff alike powered through the changes in guidance and adapted their services so they could provide the valuable care needed to those most vulnerable.
One of the biggest frustrations felt by care providers is the disparity between the attention on the potential consequences of VCOD for the NHS, compared to social care, despite the latter already operating in the midst of the measures. The Government often fail to remember that a correctly funded and resourced care sector could be one of the main support structures for a healthy NHS and therefore should be treated as an equal partner, not a guinea pig for testing the waters for new policy.
Listening to the care sector on vaccinations
To revoke VCOD, the Department of Health and Social Care (DHSC) announced another consultation, despite the Government’s clear intentions. Although the consultation has now ended (lasting one week from the 9th to the 16th of February), it begged the question of why care providers should play along. Knowing that their response would not affect the overall outcome of the consultation, they would have been using precious time that could have been better spent delivering care.
From the two previous consultations for VCOD, it was clear that the idea of mandatory vaccination would have crippling effects on the sector. In the first consultation, 75 per cent of the sector overwhelmingly opposed the measure, with Care England’s view being it should be down to the provider to decide whether mandatory vaccination should be enforced.
Despite continuously stating the negative impact VCOD would have on the care sector, DHSC refused to alter course, creating a huge increase in workload cost and stress for care providers and their employees. The care sector, like the NHS, is not opposed to vaccines and the time and resources used to ensure organisations were in line with VCOD could have been better spent persuading staff to get vaccinated. There is now also the possibility that we will see a higher number of employees resistant to getting their booster as a long-term consequence of VCOD. DHSC estimated that the introduction of the policy would have resulted in a one-off cost to care home providers of £100 million. It should now look to compensate providers for their individual losses resulting from VCOD, given the stress and anxiety they have been put through.
There is also no guarantee that this is the end of vaccination as a condition of deployment. Due to the nature of viruses and mutations, the policy may need to be brought back in. Although this scenario is unlikely, it cannot be ruled out given the turbulent times and the confused policymaking from the Government. We expect that going forward, the Government treats the care sector with the respect it deserves, listens to care providers on important issues and values them as equal partners in the health and social care sector.
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
If you disable this cookie, we will not be able to save your preferences. This means that every time you visit this website you will need to enable or disable cookies again.
Newsletter
Get a weekly update of the latest news, insight and analysis from ICJ delivered straight to your inbox!