King’s College London becomes first to benefit from two whole-body PET-CT imaging systems
By Integrated Care Journal
As part of the National PET Imaging Platform, King’s College London will support transformational research to improve the calibre of care across the UK, including providing new insights and enhancing the development of drugs and diagnostics for conditions including cancer, cardiovascular and neurological diseases.
King’s College London (Kings) has become the first site in the UK to benefit from two Biograph Vision Quadra systems from Siemens Healthineers, marking a new era of PET-CT. This crucial, non-invasive imaging technique can detect diseases’ early onset, accelerating quality of care for patients while also enabling King’s to conduct innovative radiopharmaceutical, basic science and clinical research.
As part of the UK’s first-of-its-kind National PET Imaging Platform (NPIP), a collaborative initiative bringing together transformational research for clinical discovery, King’s will use the whole-body PET-CT systems for research to improve the calibre of healthcare across the UK.
With PET-CT demand rising nearly 10 per cent annually, this technological upgrade will help King’s meet this demand and significantly expand clinical and research capabilities, positioning King’s at the forefront of global PET-CT research. With higher sensitivity than existing technology, the hospital’s whole-body PET-CT scanners will provide unprecedented insights into anatomy, improving the detection, diagnosis and treatment of complex, multi-organ diseases.
Beyond supporting NPIP, the systems will bolster complex radiopharmaceutical production and tracer development research at King’s (one research tracer production can be used for twice as many scans). Patients will benefit from improved image quality and speed of examination, while a reduction in dose will enhance paediatric diagnostics and treatment.
The UK’s adoption of whole-body PET-CT signifies a major leap forward in medical imaging, promising significant improvements in patient care and research capabilities. Funding for the first installed scanner was secured from the Medical Research Council (MRC), with the system jointly managed by King’s and Imperial College London, scientific co-applicants alongside the King’s team. The second system is financed through a strategic investment by King’s.
Image caption: (L) Peter Kyle – Secretary of State for Science, Innovation and Technology; (R) Professor Sebastien Ourselin, FREng, FMedSci, Assistant Principal (Innovation) at King’s College London visit St.Thomas’ Hospital to launch the NPIP-funded whole-body PET-CT scanner from Siemens Healthineers.
The two whole-body PET-CT systems at King’s are two of four across the UK supporting NPIP, all of which are supplied by Siemens Healthineers. By facilitating access to whole-body PET-CT imaging for clinicians, academics and industry, NPIP is set to accelerate discoveries, leading to more advances for UK researchers and better outcomes for patients. This not only enhances the UK’s clinical infrastructure but also reinforces its position as a global leader in medical technology and research.
Equipped with technical precision that redefines molecular imaging and optimises operational performance, the Biograph Vision Quadra systems from Siemens Healthineers enable near real-time imaging of a patient’s entire body. With an in-depth look at how the body interacts with administered substances, tumours can be characterised allowing for more personalised and precise treatment.
“Whole-body PET-CT has been an area of exciting development and exploration for several years now,” commented Professor Alexander Hammers, Head of the PET Imaging Centre, School of Biomedical Engineering & Imaging Sciences at King’s College London.
“We were very proud to obtain research funding for one whole-body PET-CT system; having a second one on the same site available for clinical use signifies a fundamental milestone in the advancement of nuclear medicine. I am looking forward to enhancing our research activities and our clinical services with two of these innovative scanners.”
“The addition of two new cutting-edge whole-body PET-CT scanners in our PET Centre makes us proud and excited,” added Professor Sebastien Ourselin, FREng, FMedSci, Assistant Principal (Innovation) at King’s College London.
“They will create an incredibly unique setting for the benefit of our patients, and for scaling up research and collaboration endeavours in partnership with Siemens Healthineers.”
Ghada Trotabas, Managing Director of Siemens Healthineers Great Britain and Ireland, stated: “We are honoured to collaborate with King’s College London in their ongoing pursuit to advancing molecular imaging. The installation of two Siemens Healthineers Biograph Vision Quadra systems marks the beginning of a new era in PET-CT imaging, paving the way for groundbreaking advancements in both clinical research and patient care.”
Lead image caption: (From left to right) Giulia Ginami – Strategic Partnerships Manager, Daniel Darian – Collaboration Manager Molecular Imaging, Graham Plant – Head of Diagnostic Imaging at Siemens Healthineers Great Britain & Ireland, Professor Alexander Hammers – Head of the PET Imaging Centre at the School of Biomedical Engineering & Imaging Sciences at King’s College London, Ghada Trotabas – Managing Director of Siemens Healthineers Great Britain & Ireland with one of the two new Biograph Vision Quadra systems at St. Thomas’ Hospital.
The value of partnerships in enabling holistic diabetes care
By Navodi Kuruppu
PPP’s Director of Market Access and Policy, Ameneh Saatchi, spoke with Naj Rotheram, Medical Lead for Partnerships at Boehringer Ingelheim, to discuss their view on primary care, partnerships and how they can best support the NHS in delivering a new holistic approach to diabetes care.
The Diabetes Care programme has been sponsored by Boehringer Ingelheim. Boehringer Ingelheim has had no influence over the agenda, programme development, content or selection of faculty. This Editorial was written by PPP but features content from an interview with Boehringer Ingelheim. Boehringer Ingelheim has therefore reviewed the content for factual accuracy only.
Since their establishment in 1885, Boehringer Ingelheim has evolved into a leading manufacturer of pharmaceutical drugs for both human and animal healthcare. As a research-driven company operating in the UK among many other countries, Boehringer Ingelheim aims to support the NHS in improving clinical outcomes, access to evidence-based care and the quality of life.[1] To make this happen in diabetes care, Boehringer Ingelheim researches and develops innovative medications to support patients throughout their care journey.[2]
Naj Rotheram is Medical Lead for Partnerships at Boehringer Ingelheim. Having worked in the NHS for fifteen years before joining industry thirteen years ago, her experience makes her well-placed to understand how the NHS can deliver successful holistic care to people with diabetes. In her current capacity, Naj collaborates closely with the NHS across all disease areas, including diabetes, to address challenges and improve patient outcomes.
Developing preventative, holistic care
Naj describes a now familiar picture of the NHS: a system burdened by resource constraints, backlogs, workforce pressure, low morale – issues that have been further exacerbated following the COVID-19 pandemic. These challenges have dominated health discourse in recent years, and were recently highlighted in Lord Darzi’s independent investigation, with political figures warning that the system will collapse without reform. In view of this fact, Naj has long advocated for a structural transformation within integrated care systems (ICSs) to enable entire care pathways to deliver care collaboratively and holistically, treating patients as a whole rather than focusing on a single diagnosis.
“The long-term goal of structural transformation is to support better integrated care and therefore a better patient experience, hopefully across the entire pathway and better working together. But it does take time for that integrated way of working to embed itself.”
ICSs were set up with the aim of improving health and care services, prioritising a focus on prevention, better outcomes and reducing health inequalities. The power of prevention in diabetes care has already been demonstrated by the NHS-funded Diabetes Prevention Programme, which has been shown to reduce the risk of type 2 developing by 40 per cent. Yet, a study by The King’s Fund has found that local systems are at risk of going ‘off-track’ due to pressures on services, intense political scrutiny, and extremely difficult economic circumstances – and the impact these conditions are having on the ability of local, regional and national leaders to act.[3]
The challenge for ICSs is reflected in diabetes prevalence and linked co-morbidity figures, which are continuing to rise. Since 1996, the number of people with diabetes in the UK has risen from 1.4 million to more than 4.8 million and is estimated to reach 5.3 million by 2025.[4] The challenge of a growing at-risk cohort is compounded by an ageing population, and the complexities linked with long-term diabetes management, including complications and multimorbidity cases. Recent data from the 2023 National Diabetes Audit shows that more than 3.5 million people registered with a GP were identified with non-diabetic hyperglycaemia, also known as pre-diabetes. [5][6]
Diabetes often “starts with one diagnosis,” explains Naj, “and then accumulates a host of other health risks and problems”. In fact, diabetes is the leading cause of blindness in working-age adults, and around 10 per cent of diabetes patients will develop leg ulcers at some point in their lives.[7][8] Naj’s ideal vision is a model of localised care, centred on early diagnosis, better prevention and early intervention, thereby reducing the risk of these complications developing. Central to this approach is including patient perspectives to better understand their experiences. Naj also emphasises the importance of involving primary care professionals, ICS leaders, commissioners, and national policymakers in the development of multidisciplinary, holistic care pathways.
“Patients want to be treated by someone who considers the impact that disease might have on their heart, on the kidneys, on their brain, on their eyes. They say, ‘please look after me as a whole person,’ but the NHS isn’t necessarily well set up for that.”
-Naj Rotheram
Diabetes outcomes are significantly impacted by health inequality, with rates of undiagnosed diabetes being twice as high in areas in the lowest Index of Multiple Deprivation quintile compared to the top.[9] Naj stressed the importance of harnessing and embedding data-driven insights from population health management (PHM) into diabetes care pathways to allow systems to identify, and target interventions towards, underserved communities. An example of this is the Joint Working Project between Boehringer Ingelheim Limited and Salford Care Organisation.[10] The project aims to implement an integrated, neighbourhood-based, holistic diabetes service to address the complex needs of patients with cardio-renal-metabolic (CRM) diseases in Salford. By employing a workforce with diverse skillsets, and using data to identify individuals with the greatest needs, the project has successfully engaged communities within Salford’s population that have traditionally been reluctant to participate in healthcare.
“Utilising the insights at a very local level can help us understand the challenges affecting specific areas and allow us to develop programmes and care pathways.”
-Naj Rotheram
ICSs have a range of assets available to build more holistic, preventative diabetes care. Utilising all of general practice, community pharmacy, dental services, and optometry, primary care is in a strong position to deliver comprehensive, holistic diabetes care. However, Naj points out that current support for primary care is inadequate due to limited resources and high patient volumes – leading to a more reactive rather than a preventative approach. This means that primary care is often an underutilised preventative asset.
To remedy this, Naj advocates for greater support in terms of resources, training and action on workforce sustainability. “Primary care should feel valued; they are working on issues that matter to patients,” says Naj. “These primary care healthcare professionals are making a difference at a community level, and this long-term holistic focus is the reason why they entered the profession in the first place.” Naj also discusses the importance of supporting and valuing the workforce’s skills, by addressing discrepancies in workforce development, job reimbursement, and fair pay. An international survey has found that primary care doctors in 10 high income nations say that they are overworked, demoralised, and undervalued. [11]
The value of partnership
Another often underutilised asset in improving diabetes care is industry partnership. The NHS and pharmaceutical industry have an opportunity through partnership to redesign local and national pathways, enabling better collaboration for the patient’s benefit. Alongside clinical and care pathway knowledge, industry partners offer a range of practical resources and expertise relevant to NHS system ambitions, including project management, stakeholder involvement and multidisciplinary team mobilisation.[12] Naj has been intimately involved in this work, and posits partnerships as one way of promoting ethical practices and to provide highly regulated and standardised settings in which the NHS and industry can operate. Naj believes that partnerships can help to improve trust between the NHS and industry through greater transparency regarding all parties’ actions, long-term motivations and impacts. For this reason, the NHS could rely more on the “tremendous” skills and resources that industry brings, which extend beyond just the financial resources it provides.
We need to embrace working together and pooling those skills and those resources to overcome some of the NHS challenges that we are collectively facing.
-Naj Rotheram
PPP’s Diabetes Care Programme 2024 has uncovered fascinating insights and developed vitally important recommendations to improve the delivery of diabetes care. Stakeholders and experts present across the roundtables have consistently highlighted the need to move away from treating diabetes as a single diagnosis and condition to treating the whole patient in holistic terms.
The theme of holistic care has shaped the basis of 2025 Diabetes Care Programme, Holistic approaches to diabetes care: treating the whole patient, to discuss the challenges and opportunities for a holistic approach to care that treats the ‘whole’ patient and not just their diabetes. The series will feature a set of roundtables to create insights and strategies for holistic approaches to diabetes management and long-term conditions. We will address key questions including:
• How can systems balance personalisation and population health management to ensure we get population health rights, while meeting the individual needs of people?
• What role can technology, data and digital play in reducing inequalities for those with the highest needs?
• What innovations are game changers and are they sustainable?
• How do we develop our prevention and risk strategy, to break down siloed disease working so that cardio, renal, and metabolic condition are joined-up effectively within the health and care system?
• Where are the overlaps within the multi-morbid patient population and how can we create a one-stop shop in the community?
• How significant is genetic predisposition in causing diabetes compared to dietary and environmental factors?
If your organisation would like to learn more about getting involved in this innovative programme, then please contact Ameneh.saatchi@publicpolicyprojects.com to find out more.
By Leanne Stevens, Abbe Ruston, Laura Hallas Hoyes
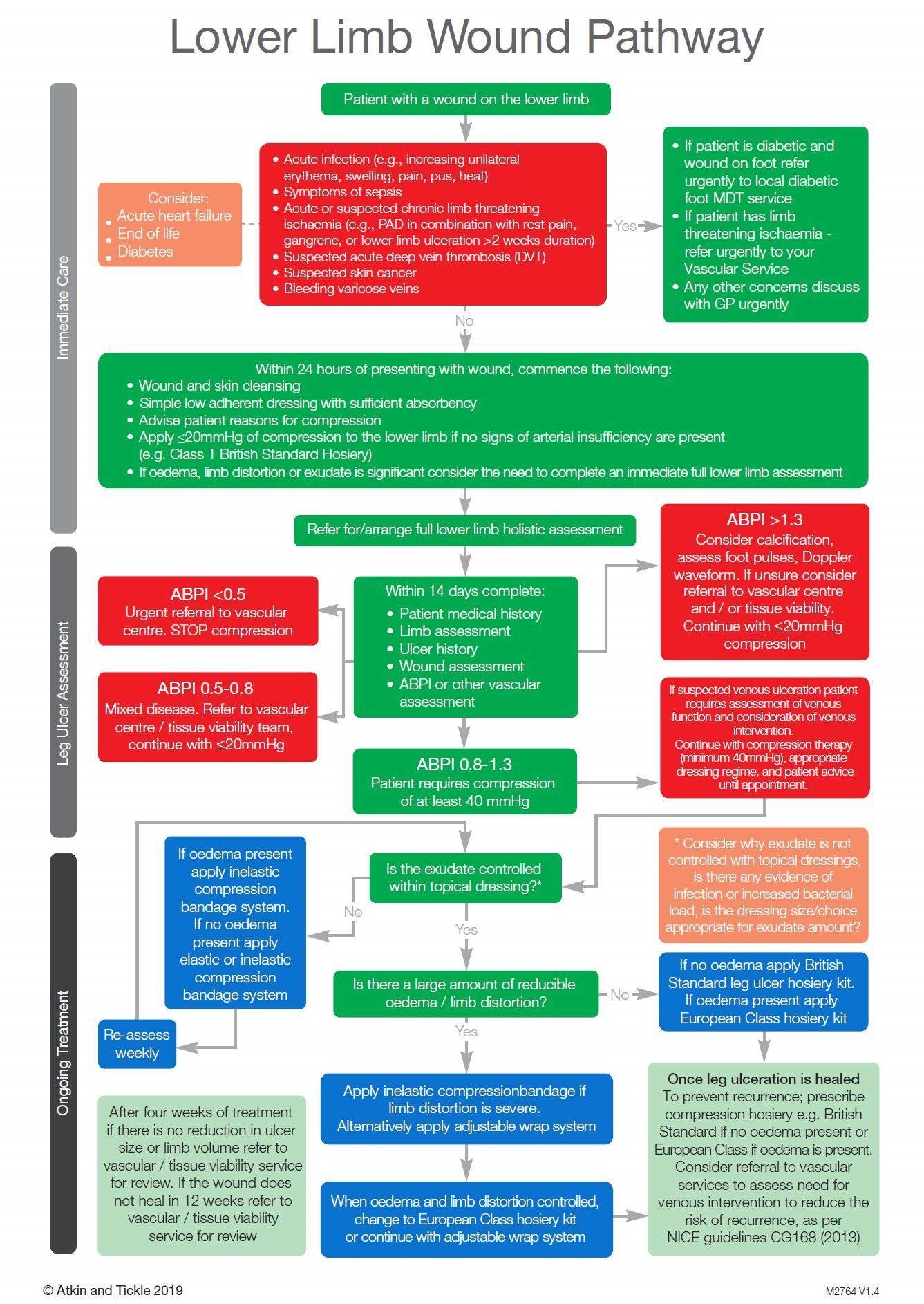
It is estimated that more than a million people in the UK have lower limb ulceration. With their 160 years’ experience in developing wound care solutions, L&R hypothesised that a self-care delivery model could both improve outcomes and ease the burden on the healthcare system.
L&R has more than 160 years of experience in developing outstanding wound care and compression therapy solutions. They are passionate about transforming outcomes in leg ulcer service provision to support the NHS, the nursing workforce, and patients. Working in partnership with organisations, L&R supports them to drive the self-care agenda, which frees up resources, reduces appointment times and clinic costs, and releases nursing time to care.
Lower limb ulceration is a common cause of suffering in patients and its management poses a significant burden on the NHS, with venous leg ulcers (VLUs) being the most common hard-to-heal wound in the UK. It is estimated that more than one million people in the UK have lower limb ulceration, of which 560,000 are categorised as VLUs. Much of burden of VLUs currently sits within the community and primary nursing workforce, with up to 50 per cent of community nursing workload being taken up by chronic wound management.
In South West Yorkshire Partnership Trust (SWYPT), it was hypothesised that a self-care delivery model, in partnership with the Leg Ulcer Pathway could reduce wound care burden on the health service and improve patient empowerment, with little or no reduction in healing outcomes.1 Therefore, L&R, in partnership with SWYPT, created a project called the “Big Squeeze”, with the aim of delivering transformative outcomes for venous leg ulcer care, achieving a big squeeze on its financial burden and unwarranted variation in treatment and outcomes.
This was implemented through L&R’s three-step approach:
Implementation of a best practice leg ulcer pathway1 – ensuring the right treatment for the right patient at the right time in line with the National Wound Care Strategy Programme recommendations.
Service efficiencies – driving clinical and health economic outcomes through adoption of the self-care delivery model.
An education and coaching programme – for patients and clinical workforce to embed sustainable practice.
Click to enlarge
Evidence of success
95 patients were enrolled into the service evaluation, and:
VLUs of 84 patients had healed by week 24 on the pathway.
VLUs in a further 10 had healed by week 42.
One remaining patient reached 42 weeks without healing.
Comparing the results of implementing the Best Practice Leg Ulcer Pathway in isolation and the Best Practice Leg Ulcer Pathway and the Self Care Delivery Model combined:
Nursing hours per patient reduced from 24.5 to 1.3, releasing up to 95 per cent in nursing hours.
Total cost per patient reduced from £2,168 to £361, saving up to 83 per cent in total cost of care per patient.
Product cost per patient reduced from £629 to £177, saving up to 72 per cent in product costs per patient.
In addition to healing and financial outcomes, improvements in staff motivation and wellbeing were recorded through survey feedback, as well as 1,471kg saving in C02 per 100 patients through a reduction in miles driven by the community workforce.
Creating a data-driven health organisation across Milton Keynes
By Oracle Health
Between 2018 and 2023, Milton Keynes University Hospital NHS Trust gained a large set of clinical data. On its journey with Oracle Health, the trust has transformed into a data-driven organisation, improving patient experience, lowering the cost of care, enhancing the staff experience, improving population health, and addressing health equity.
What’s the background and context?
Over the past few years, Milton Keynes University Hospital NHS Foundation Trust (MKUH) has been on a clinical digital systems journey. Due to the recent advances in the organisation’s Oracle Health (formerly Cerner) electronic patient record (EPR) system between 2018 and 2023, they have gained a large set of clinical data. This has enabled MKUH to make strides in visualising and using information to support the Quintuple Aim, which includes improving patient experience, lowering the cost of care, enhancing the staff experience, improving population health, and addressing health equity. MKUH continues to advance in this field, with its goal being to evolve from a data-driven organisation today to analytic excellence in the future.
Using data to drive EPR adoption and help improve patient outcomes
MKUH had historically hoarded data and used information for outputs including statutory and ad hoc reports. However, with limited resources, the Trust struggled to find the right information for the right end users. Their data workforce and skill set were designed based on needs of traditional NHS statutory reporting, so using data more directly as an enabler for improving staff experience and patient health outcomes was an alien concept.
There was a gap between teams that needed to manage the data and format it in a way that made it meaningful and useful to those making clinical or operational decisions. The way MKUH accessed the data was down to the end users using the system and understanding the workflows. In the initial stages, once data had been clinically validated, the team could create dashboards for a small subset of users.
A dawn happened when Cerner Millennium was connected directly to the Trust’s PowerBI instance, a Microsoft product that allows users to pull in data and information to produce dashboards and visualise data in a way that’s meaningful and insightful to the end users. As PowerBI is used across the Trust for a multitude of purposes, including this data within the same platform enabled a more seamless user experience. Creating dashboards of rich data is academic if they are unusable.
Ways data is being used to drive the organisation
The very first project to use data differently analysed the way MKUH was receiving pathology and imaging results in Cerner Millennium, and the process of endorsing those results. This was a real technological response to an organisational need. Electronic endorsing of results was, at the time, a new concept that MKUH clinicians had variably adopted. There was often discussion about how electronic endorsing could be improved. How do we improve adoption, and how can we measure it? How do we know who is and isn’t endorsing results? How do we know we’re improving it? This became a sticking point, and the hospital didn’t know how to move forward.
Presenting the data through PowerBI enabled the team to split the data by department or lead clinicians responsible for results, allowing them to share the report with clinicians. Through PowerBI, it’s also possible to give access to the full report – with snapshots once a month – so each lead clinician or department could see how they’re doing, with a league table. After examining the data, the team decided to set a target: 80 per cent of results would be endorsed within two weeks. They then discovered the data included encounters for consultants who had previously left the organisation, which prompted MKUH to look at their leavers processes. For example, what steps must be taken when a clinician leaves?
Many results were attributed to senior nurses and midwives, which prompted the team to bring them into the fold in conversations and, if appropriate, have them endorse their own results. Occasionally, clinicians were ordering in the wrong encounter, which would then associate the wrong lead clinician with it. Having the data has shed fresh light on the process, and MKUH has discovered much more than it anticipated. It took time to organise this dataset, with completion only coming about in 2020 following the 2018 go-live. The team did several things wrong and made mistakes before they were able to share the correct data on endorsing results.
The next big phase was development work in response to the challenges presented by the COVID-19 pandemic. At its onset, MKUH was still an organisation driving the need for data, as opposed to being a data-driven organisation. The Trust was eager to see the data, which enabled it to prioritise the work. By compiling the data, the team had a new technical skill set across the department, but the real challenge was understanding the dataset – bridging the gap between understanding workflows and managing data.
The team experimented with the COVID-19 data, which provided several different visualisations. Two years into the pandemic, they were using the fifth version of the dashboard, which allowed them to view patient cohorts by postcode, interrogate cases of nosocomial infection (hospital-acquired COVID-19 infections) in patients, and look at those patients’ location histories – including their previous wards and beds, and which other patients they may have been in contact with.
Specific views of this report were also provided to Milton Keynes and Buckingham local health teams, with shared data sorted by relevant postcodes. These reports were updated daily, and team feedback showed that the information shared was very helpful. In December 2020, MKUH was part of the first wave of COVID-19 vaccination centres and utilised the Cerner mass vaccination workflow, Microsoft booking application, and PowerBI to create twice-daily site reports. These reports flagged data quality issues, monitored progress through the vaccination centre, and provided metrics – regarding the number of patients vaccinated, how many patients were waiting, and so on.
COVID-19 was the first time the team focused on building a system that was conducive for reporting and sharing data, and the first time data drove the way the system was built.
Designing the system with data in mind
An example of designing the system with data in mind is the revaluation of free-text fields where users can add unstructured text. MKUH knew it would require time investment to make changes. For example, MKUH reviewed a midwife form used to record patient birthing preferences. Assuming the form was completed, no action was taken, nor did the data go anywhere. MKUH redesigned the form entirely, with data in mind. Answers to questions now populate the antenatal document, meaning anyone who treats patients can view, and take into consideration, their birthing preferences. The nature of the form was then changed so it was rendered into textual narrative document and easier to consume.
Currently, reporting is available to the midwives – refreshed daily to show the number of forms completed and by which midwife. The Trust then uses this data to target extra training. For instance, it’s important for the rendered note to be completed, as this document is shared with the patient through the MyCare patient portal. When reviewing the reporting, if the Trust sees more forms than completed notes it follows up with the midwives, reiterates the process, and ensures they complete the two-step process so they can create the note again.
MKUH can then report on the number of booked patients who are more than 34 weeks pregnant and have no birthing preferences noted. This highlights gaps in the process and enables the Trust to follow up with patients to ensure their information is complete at the time of delivery. Capturing this level of data also enables the Trust to gain a better understanding of the birthing preferences of the Milton Keynes population. All of this is possible because workflows were designed with these data aims in mind, rather than being an afterthought. In simple terms, the report was designed before the data-capture forms.
MKUH has started a journey with the Oracle Health Command Centre, including real-time, predictive analytics using AI. This takes a dataset from historical EPR statistics and allows the organisation to review real-time statistics with added predictions on the hospital bed state in four-, eight-, or 12-hour intervals. This was only recently implemented, so as MKUH continues to progress, the Trust will assess the predictions accuracy and then work to update the algorithms to better align with actual events.
There are also other pilots exploring how to better use data within buildings and the hospital environment. MKUH didn’t know how its wards and spaces were being used, and with upcoming building projects, there were opportunities to take a data-driven approach to hospital design and ergonomics. As there was no existing way to accurately manage this, MKUH worked with partners Haltian and their Empathic Building solution to track staff movements – with permission – and equipment around a particular ward. By starting with the question, the organisation wanted to answer, MKUH could then build a solution that captures required data and presents it in a manner that allows management to make more informed decisions about the future hospital design with patients and staff in mind.
How does the NHS culture need to change?
National datasets feed into decision-making at a regional and national scale more generally, and into commissioning more specifically. There will always be a place for this mechanism, even if it could benefit from a little pragmatic consolidation.
When a hospital is reactive to local, regional, or national targets, the effort invested in reporting against those targets is increased and improvements are generally seen in that area. There’s a clear cost versus benefit case for the invested time and effort that brings in roles from all parts of the management structure; financial incentives are a big driver for this activity.
Finding alternative ways to commission hospitals so incentives are different but just as attractive has been a more recent approach and represents a move away from pay-as-you-go. If this were done in parallel with reducing how prescriptive that commissioning activity is, providers are afforded the space and incentive to be more innovative in the ways they deliver services. Were there support on how to introduce those innovative models into hospitals – whether exemplar sites, services, or cases that used information to respond to this challenge successfully, access to models or approaches that can be applied locally, or short-term training offered by NHS centres of excellence to develop the skills to lead on such work – then there could be a culture shift. This would be contingent on local efforts bearing fruit, so end-to-end support would be needed.
The world of information governance has come so far since COVID-19 and the introduction of the EU General Data Protection Regulation (GDPR). It is important that an information governance program considers events that can impact the organisation and legal requirements, while also considering operational efficiency. The work done across OneLondon, the Wirral, the Great North Care Record, and many more demonstrates information governance is possible and doesn’t need to be restrictive.
It’s not just NHS culture that must change. Hosting data and information management functions no longer needs to be an extortionately expensive offering. However, the commercial, well-known products available to the NHS for this purpose remain at inflated costs – leaving many to keep what they have, make difficult decisions to spend money on these platforms instead of direct care, or try to use local in-house solutions or open-source options that require significant in-house expertise.
MKUH is developing a growth culture as it responds to having data available to drive organisational change. This culture change is in progress and this case study highlights some of the benefits being realised and the ideas being explored.
Rethinking cancer care: a system strategy for improved outcomes
By Lucia De Santis and George Batchelor
Boosting early detection and reducing backlogs through data-backed, collaborative initiatives will be crucial to addressing the deteriorating state of cancer care in the UK, write Edge Health’s Lucia De Santis and George Batchelor.
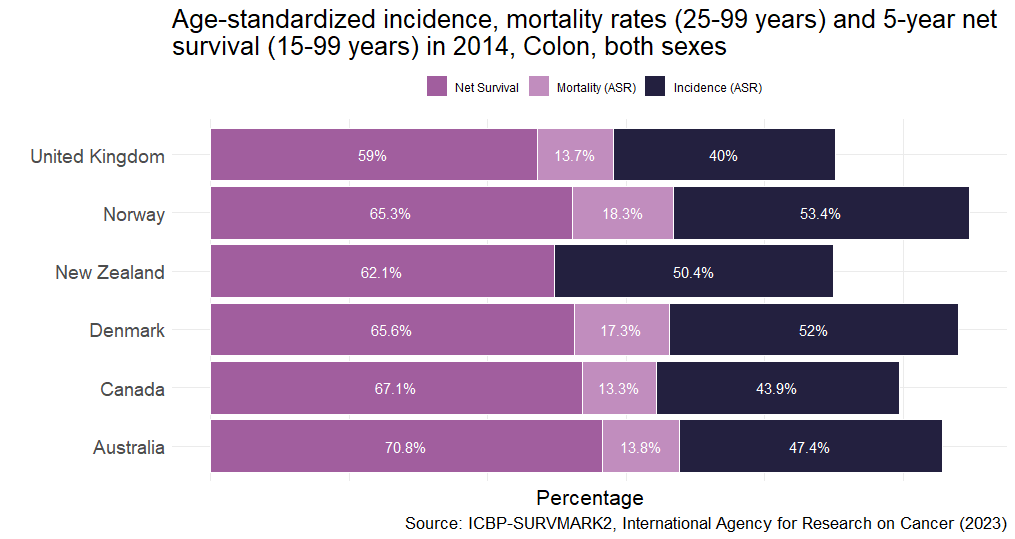
In the battle against cancer, the UK is grappling with alarming statistics, with outcomes for colon, lung and pancreatic cancers being particularly sobering. According to the Comparator report on cancer in Europe 2019, the UK was last out of all Western European nations for 5-year survival of colon cancer, as well as among International Cancer Benchmarking Partnership (ICBP) jurisdiction countries (Figure 1).
Figure 1: Age-standardised incidence, mortality rates and 5-year net survival for Colon cancer. Arnold M, Rutherford M, Lam F, Bray F, Ervik M, Soerjomataram I (2019). ICBP SURVMARK-2 online tool: International Cancer Survival Benchmarking. Lyon, France: International Agency for Research on Cancer. Available from: http://gco.iarc.fr/survival/survmark, accessed [08/06/2023]. (Click to enlarge)
The complex factors behind the UK’s cancer outcomes
Understanding the root of this crisis is not straightforward, as many intertwined factors play roles, from cultural attitudes affecting help-seeking behaviours to underinvestment in critical medical resources. As a doctor in a busy acute trust, I could not grasp why one of my patients only presented to hospital long after his skin tone had turned an unmistakable dark shade of yellow, a tale-telling sign of his late-stage lymphoma. On the other hand, as of 2021, the NHS operated with around 63 decade-old LINACs (essential cancer treatment machines), and the UK has the lowest number of PET-CT scanners per 100,000 people among International Cancer Benchmarking Partnership countries.
The UK’s uphill struggle is deep-seated, with it having the worst cancer survival rates in the EU as far back as 1995. NHS’s low spending on cancer treatments and restricted access to cancer medicines for patients have been contributing factors.
Turning the tide: a dual-pronged strategy
Despite the complexity, there are attainable starting points for improvements: boosting early detection through the two-week-wait (2WW) referral pathway and ensuring prompt diagnosis and treatment through collaborative approaches that have proven successful in other countries.
Front one: boosting early detection
Data shows that cancers identified via a 2WW referral are often diagnosed earlier, and result in fewer diagnoses during emergency admissions, with implications for survival.
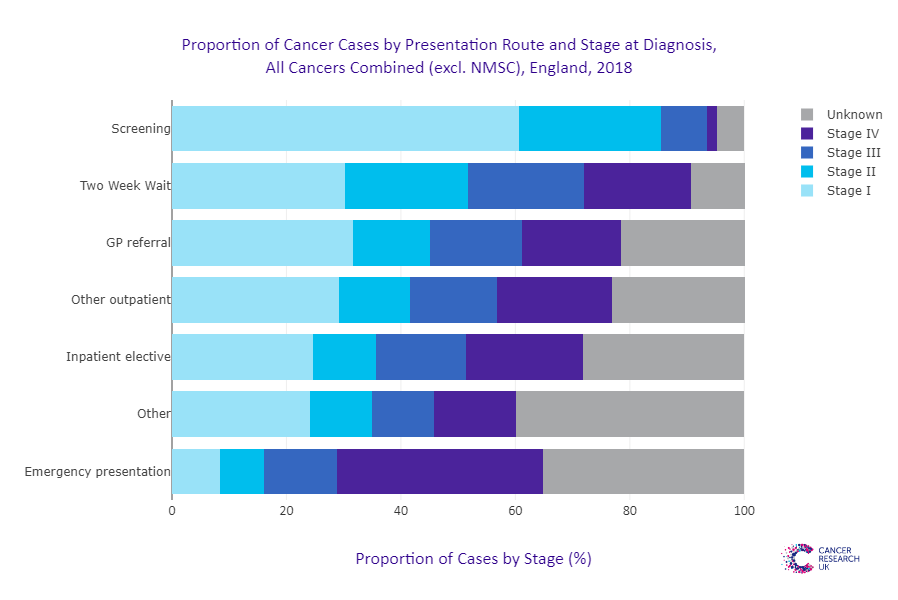
Analysis on stage at diagnosis performed by Cancer Research UK (Figure 2) demonstrates this clearly, with 30 per cent of cancers detected via 2WW referral being at Stage 1, versus just 8 per cent of cancers detected through an emergency presentation to hospital.
Figure 2: Proportion of cancers by stage at diagnosis by route of detection. Source: Cancer Research UK Early Diagnosis data, accessed June 2023. (Click to enlarge)
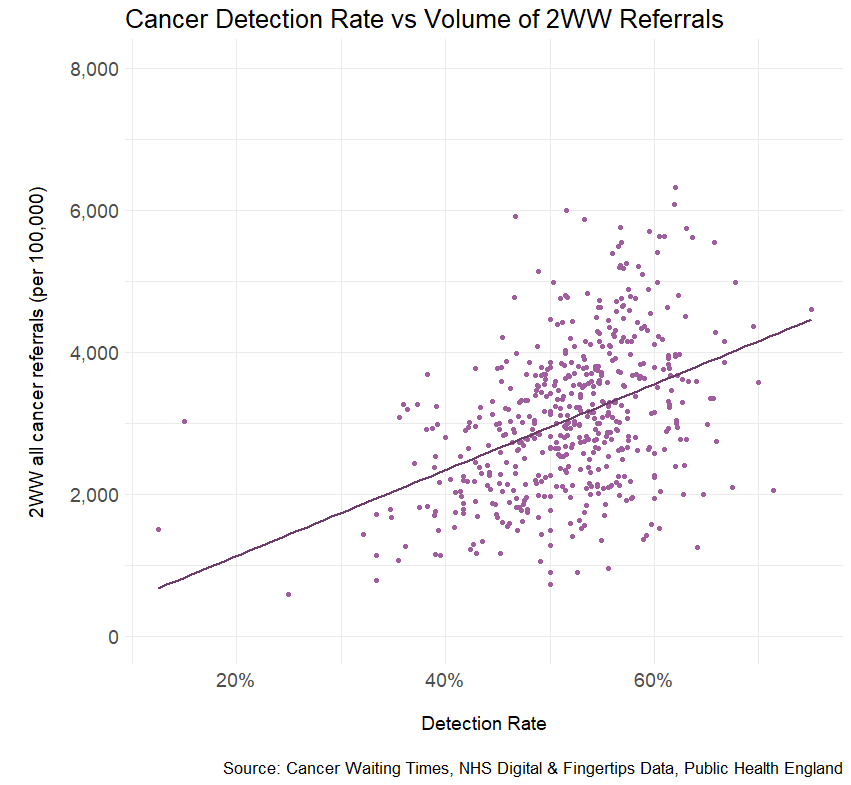
However, across England, there is a glaring disparity in cancer detection rates – that is, the number of confirmed cancers that are detected via an urgent suspected cancer referral (2WW). This is intimately related to the overall volume of 2WW referrals (Figure 3), where higher figures are associated with a higher detection rate.
Figure 2: Proportion of cancers by stage at diagnosis by route of detection. Source: Cancer Research UK Early Diagnosis data, accessed June 2023. (Click to enlarge)
Patients whose practices have a lower threshold to refer under the 2WW programme fare much higher chances to have cancer detected via this route and as shown above, at an earlier stage. This, again, has implications for treatment and survival.
The national disparity between these practices not only means that average figures for cancer outcomes are affected by differing primary care strategies, but also that there are wide inequalities of care across the nation.
Cancer alliances and primary care networks can play an essential role in encouraging practices to revisit their referral behaviours. This effort can help reduce healthcare inequalities and potentially save lives by identifying and treating cancer earlier. Understanding what drives referral rates and promoting effective referral practices can make the difference between a life saved and one lost, and in the end spare the much higher healthcare and societal costs associated with late-stage cancer.
Front two: tackling backlogs through collaboration
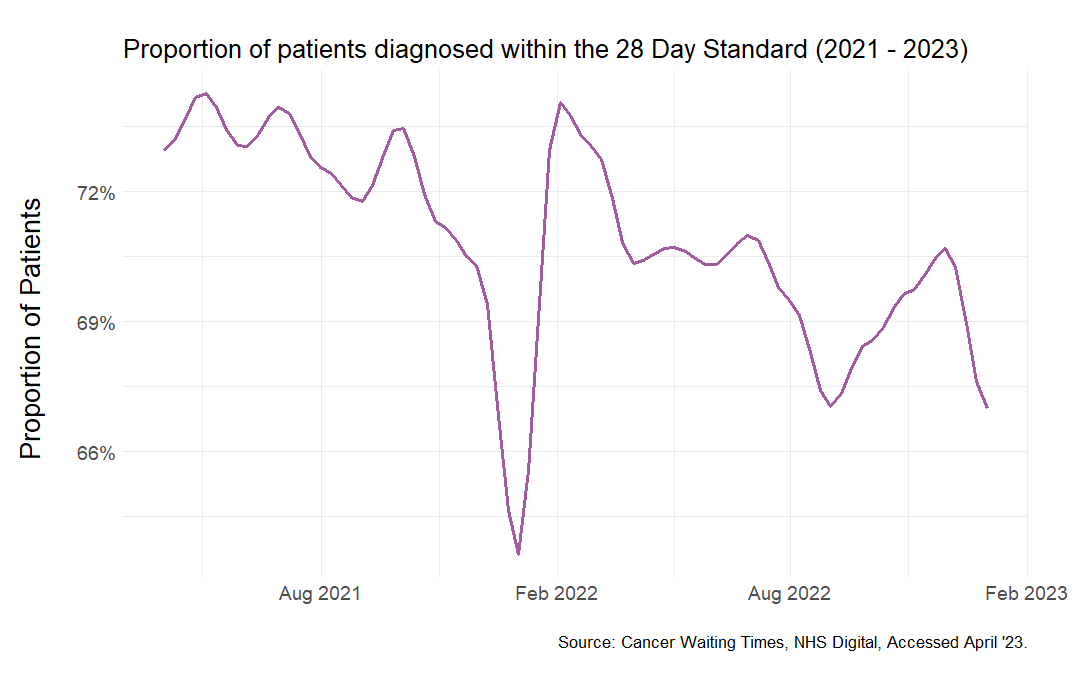
Our second strategy is to reduce backlogs through collaboration. The NHS’s diagnostic capacity is currently strained, as the steady decline in patients diagnosed within the 28-Day target since its 2021 introduction suggests.
Figure 4: Proportion of patients referred for suspected cancer who meet the 28-Day faster diagnosis standard that was introduced in 2021. (Click to enlarge)
Taking cues from countries like Denmark, which successfully improved cancer survival rates by centralising specialised care and launching data-focused initiatives, the NHS can rethink its approach. By making comprehensive cancer patient data centrally available, we can make more informed decisions, improve workflow, and direct finances more effectively.
The NHS collects extensive data on cancer patients, encompassing their entire journey from referral to treatment. The key to better cancer care is ensuring the data is available centrally to key organisations and decision-makers, such as integrated care systems and Cancer Alliance leaders, to make evidence-backed financial, workflow and population health decisions and foster collaboration.
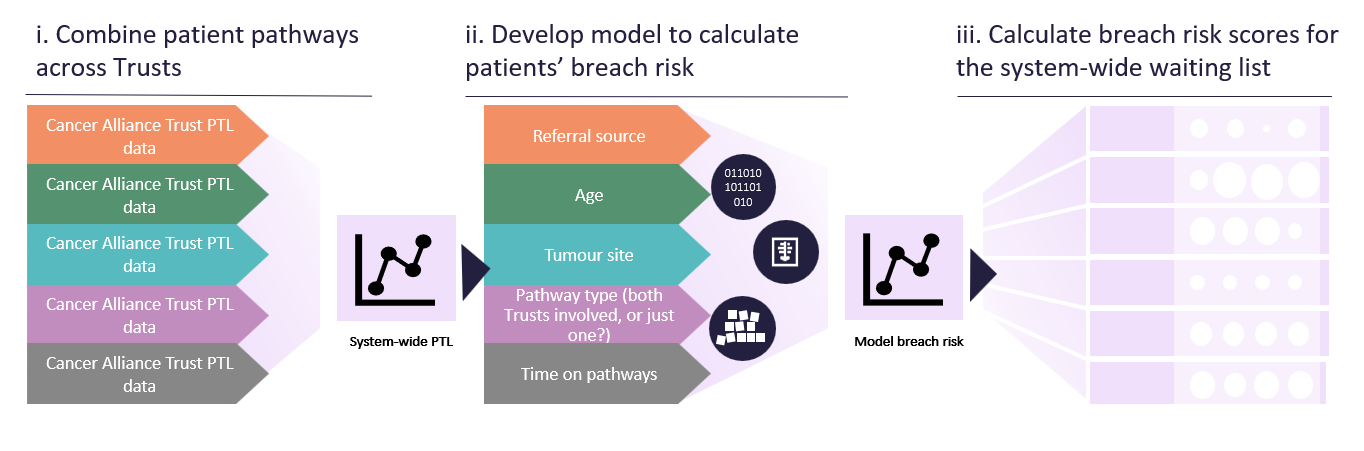
Sharing cancer data can help speed up diagnosis and treatment for patients. For instance, by sharing a cancer patient tracking list (PTL) across multiple trusts, patients who are at risk of breaching targets can be identified early and receive timely care. This strategy can also address the shortage of diagnostic appliances or services and specialised treatment.
Figure 5: Example of how cancer alliance PTL data could be pooled to estimate breach risk scores and inform waiting lists to either allow local prioritisation or highlight mutual aid opportunities. (Click to enlarge)
The road ahead: data-driven initiatives and collaboration
The current state of cancer care in the UK calls for an urgent, systemic response. By prioritising early detection and fostering data-driven collaboration, we can significantly enhance the prognosis for the UK’s cancer patients.
Expediting early detection efforts, particularly through increased 2WW referrals, is crucial to change the narrative. These efforts, when paired with the power of collaborative and data-driven care models, can revolutionise the cancer care landscape. It’s a potent combination that can help us ensure that no matter where patients live, they can access timely and high-quality cancer care. This system-wide approach presents an opportunity not just to catch up with our European neighbours, but to potentially lead the world in effective cancer care.
Elective backlog and care priorities: a call for localised solutions
By George Batchelor and Lucia De Santis
Edge Health’s George Batchelor and Lucia De Santis explain the need to develop localised solutions to drive the NHS’s elective care recovery.
March 2020 marked an unprecedented change in the NHS and healthcare provision. As resources were diverted to the pandemic response, virtually all elective activity ceased, and the healthcare system transformed into a huge acute response machinery. We knew this would not be a sacrifice without consequences, but it was worthy of the stakes at play – millions of lives affected by COVID-19.
Fast-forward three years: the pandemic is now over for many people, but its impact on the NHS remains. This impact goes beyond the ever-growing elective backlog to include a fundamental shift in how care is provided, as well as a host of top-down targets that place increasing challenges on care providers.
The state of the elective recovery
Many will be familiar with the dire state of waiting lists for consultant-led elective care that topped 7.2m in October 2022 – a 64 per cent increase from March 2020 and with a median waiting time of 102 days.
Amid efforts to tackle the backlog, the recovery strategy has pushed for “doing more” with an ever-increasing range of performance measures to drive increased throughput and avoid adverse incentives, including: achieving zero 65-week waits by March 2024, increasing completed pathways by 110 per cent, increasing valued activity by 104 per cent, performing all diagnostic tests within 6 weeks, and several more.
Competing targets can be confusing to navigate and add pressures to already stretched systems, but they also fail to account for novel care challenges and regional variation. Working closely with trusts and ICBs, Edge Health has encountered, again and again, a stark increase in patient complexity since the pandemic and the consequences of a depleted, exhausted workforce that don’t show up in figures and targets.
Click to enlarge image.
To add to this, Covid has also prompted a greater focus on prioritisation and clinical urgency in allocating care, as opposed to a first come, first served system, which poses added challenges in correctly allocating services when some patients have been on a waiting list for more than two years.
How targets fuel a new hierarchy of care: emergencies, long-waiters, then everyone else
Despite the impressive efforts and successes of restoring elective activity after the pandemic, as well as the rise of innovative ways to provide care and promote collaboration among providers, we are still far from having room to breathe. In this context of significant mismatch between demand and capacity, the limitations of national targets that would encourage efficient management in a balanced system are laid bare.
A pertinent example of this is elective waiting lists, which have been the object of various targets to reduce long waits. The good intentions behind these targets are undeniable; no one should be made to wait for care for more than a year. In a system where demand is matched with capacity, such long waits should never be an issue. In principle, a sudden surge in capacity directed at these long waiters might be enough – at least for some trusts – to clear them. However, this is problematic for two key reasons: it fails to account for clinical urgency and the resources that must be reserved for the sickest patients, and it directs disproportionate energy to 2 per cent of the waiting list.
Previous experience shows that initiatives to address targets are incredibly energy-consuming for trusts. They may also fail to gain buy-in when they don’t match local clinical priorities. What we have seen at large trusts is that the backlog of elective diagnostics does not stand a chance in front of the volume of emergency and two-week-wait cancer referrals. As patients approach waiting targets, however, they are pushed to the front of the queue to avoid missing them. This is not solving the backlog issue – it merely adds another pressure point.
Click to enlarge image.
Perhaps more throughput-focused national targets, such as setting a maximum number of waiting-list per head of population, would be more effective while allowing trusts to decide how to manage their own waiting lists.
ICBs create an opportunity to focus on local priorities
If there is one thing that the pandemic has demonstrated about the NHS, it is that when empowered, trusts and local systems are pioneers of innovation and can rise to unprecedented challenges. From the London Ambulance Service, which partnered with the London Fire Brigade to deal with rising ambulance demand, to the Royal Surrey NHS Foundation Trust that partnered with a local private hospital to provide excellent palliative care despite the pandemic (NHS Providers, 2020), the pandemic bore witness to numerous examples of unparalleled collaboration and innovation.
There is an inevitability about some targets in that they reflect national priorities and are a way of tracking progress and holding systems to account. There is some evidence to suggest they motivate change and can be a catalyst for improvement. But the flipside is that blanket targets don’t take into account local need and they penalise providers that are otherwise making huge progress on elective recovery. They’re also not particularly good at motivating staff in a positive way—health and care professionals understand that targets are organisationally important, but they’re not always aligned with what professionals and patients think is important. If ICBs are to be held accountable for delivering on targets, it only seems fair that they should have a say in what the targets might be and it can be expected that priorities might change from one locality to another.
This should not be seen as a limitation, but as an opportunity. We think ICBs are the key for a more nuanced approach to designing and setting priorities that might catch two (or more!) birds with one stone: managing the elective backlog and addressing local need with highly relevant targets.
ICBs could set their own targets, that are in line with national priorities but refined to fit local circumstances. Local systems could engage their workforce and patient voices in agreeing what these look like. This approach still creates accountability and sets a direction for change (the point of targets) but also gets buy-in from the teams charged with meeting the targets—targets that reflect their priorities and what they see in their own practice.
It doesn’t have to mean a free-for-all or ducking difficult problems. National bodies can still ensure local systems are ambitious, hold them to account, and provide support and guidance to deliver change. Programmes such as GIRFT do this very successfully. Instead, what we propose would allow local systems to have more freedom to invest in novel care strategies to tackle their unique challenges. Importantly, it could be a mechanism to engage with, value and retain the workforce.
Of course, the counter is that differences will emerge across localities. But the truth is that this is the current reality, demonstrated by the charts above. And those differences would likely start to narrow if – and this is critical – ICBs are given time to flourish, work to meet local priorities and learn from one another.
About the authors
George Bachelor is Co-Founder and Director of Edge Health specialising in the delivery of advisory services and data products that improve operational performance for clients in the health sector.
Lucia De Santis is a qualified medical doctor and Analyst at Edge Health, providing subject-matter expertise on the clinical/data interface and coordinating Edge Health’s thought leadership.
How IQVIA is optimising respiratory pathways to enable long-term NHS recovery
By Integrated Care Journal
As the NHS continues its recovery from Covid-19, IQVIA has been working with integrated care systems, with its analytics capabilities helping them to deliver on regional and national priorities.
The NHS has been significantly impacted during the pandemic and must prioritise workforce investment, COVID-19 recovery and a reduction in the backlog of care. To support patients, key objectives have been outlined in the NHS Long Term Plan and the NHS Operational Planning and Contracting Guidance. These objectives support the integrated care systems (ICSs) priorities to:
Enhance experience of care
Improve the health and wellbeing of the population
Reduce per capita cost of healthcare and improve productivity
Address healthcare inequalities
Increase the wellbeing and engagement of the workforce
IQVIA, a human data science company, has been working with ICSs to achieve these priorities as well as the overarching aims of the NHS. Through its Interface pharmacist team, a team of clinical pharmacists and nurses who support primary care and community health services, IQVIA can support with patient identification and treatment actions, therapy reviews, patient and clinical education and flexible capacity support.
Case study: Leicester, Leicestershire & Rutland (LLR) ICS
IQVIA were commissioned by LLR to deliver a Respiratory Optimisation Programme over a seven-week period. This clinical support was intended to ease some of the pressure caused by the backlog of care and allow vulnerable patients to receive timely support due by providing additional clinical capacity. Over the course of the programme, IQVIA were able to:
Identify opportunities for improvement, support efficient allocation of resources and deliver patient-centric services which improve access to medicines and optimise care.
Identify gaps in care, recognise patients at risk of adverse events and improve patient outcomes.
Provide skilled capacity to deliver best care at scale and address healthcare inequalities.
Provide mentorship opportunities to the multi-disciplinary team and support and sustain enhanced care.
IQVIA’s Interface pharmacists delivered 3,000 COPD clinic appointments across the LLR ICS, working with 71 practices – with 54 per cent of the pharmacy practices in the LLR ICS. Across these practices, 11,348 patients had a diagnosis of COPD recorded. 8,692 of these (77 per cent of the total) were identified as potential beneficiaries of treatment optimisation, and 7,420 of these patients (85 per cent) were invited to a COPD clinic.
Of those patients seen in clinic,
635 patients received an escalation to their current level of management
100 patients received a de-escalation of their current level of management
2,132 patients maintained their current level of management
1,119 non-pharmalogical interventions were made, including referrals for smoking cessation or pulmonary rehabilitation
Due to the pandemic and subsequent backlog in care, many of these patients had no recorded care process in the last 12 months. After the pharmacist clinics there were significant increases to these key markers, including:
A 96 per cent increase in patients who had a COPD review
A 171 per cent increase in patients who had their inhaler technique checked
A 212 per cent increase in patients with a CAT assessment
The seven-week support programme provided LLR with the additional clinical resource needed to assess and proactively manage patients with COPD. The increased capacity benefited the health and well-being of patients whilst the multi-disciplinary team were engaged with the review to provide ongoing, continued care.
About IQVIA
IQVIA utilises extensive data and analytics capabilities to inform clinical decision-making. To support and drive key advancements towards improving patient outcomes, IQVIA is at the forefront of unlocking the potential of NHS health data to realise future health improvements for the UK and deliver transformative benefits for the patients of today and tomorrow. IQVIA believes that the value of NHS health data is not in the data per se, but in the clinical decision-making it can inform. As a trusted partner to health systems and providers, we use our extensive data and analytics capabilities to transform health outcomes and deliver pioneering biomedical research within the 95 per cent of NHS Trusts who use one or more of our services.
Prevention, early access and health inequalities: Redefining place-based care
By Gavin Bashar
Gavin Bashar, UK & I Managing Director at Tunstall Healthcare, discusses the focus on prevention, early access and health inequalities and the need to use technology to redefine place-based care.
If the healthcare system is to are to re-define care and achieve preventative services that reduce health inequalities, it’s important to approach services both holistically and through targeted resolutions to specific areas of care provision.
Redefining place-based care
Place-based care has the potential to deliver multiple opportunities. In order to capitalise on those that are presented, it is important to first define ‘the place’ and what this means to people both providing and accessing care services.
When defining place-based care it’s important to consider the different demographic regions across the UK. There are disparities in the health and wellness of communities with different population characteristics, and differences in access to technology, health and wellbeing, and life expectancy should be accounted for.
By starting with place-based care, it is possible to approach issues around prevention and proactivity and the tailoring of care. This in turn will help care providers to combat health inequalities and improve access to health, social care and housing.
The implementation of ICSs
It is hoped that integrated care systems (ICSs) will drive real system change that removes silos that are currently placing barriers on delivering the most effective services.
Considering single accountability and each step of an individual’s care journey will empower us to support ICSs in their role. This will be further supported by real collaboration and integration across the system. If we address issues and demand earlier, budgets and funding streams can be allocated to the specific areas that need them.
The role of tech
Technology’s role as an enabler can move the prevention agenda forward, however it is only valuable if it drives sustainable system change. In order to integrate technology effectively, we must bring the right skill sets into our services to ensure they can deploy digital solutions successfully.
Technology can have significant benefits for citizens, particularly in terms of using data to provide intelligent insight to inform more personalised and preventative care. We should see the ongoing progress that’s been made around data privacy continue, particularly as future generations are now growing up in a digital landscape. This will lead to citizens being more comfortable with health and care technology, and having a better understanding of how they can be empowered to play a more active role in their own wellbeing.
Why interoperability is key to transforming the healthcare service and patient safety
By Ed Platt
Ed Platt, UK Sales Director for Omnicell UK & Ireland, discusses digital systems and why interoperability is key to transforming the healthcare service and driving patient safety.
Within healthcare, interoperability is the integration of technology and healthcare systems to simplify the communication, delivery and digitalisation of clinical information across an organisation or system. Effective interoperability allows for improved collaboration and clinical workflows to inform crucial decision making, creating time and financial savings – all with the aim of driving better patient outcomes.
Omnicell, as a leading medication management solution provider, is paving the way for interoperable technology to become widespread in the healthcare landscape, as it is in other sectors. Omnicell’s Automated Platforms have been integrated with several leading providers of Electronic Prescribing and Medicines Administration (ePMA) and electronic patient record systems (EPR, more commonly known as EMR outside of the UK) which have led to a reduction in medication errors and better workflows for staff.
These working interfaces are with Better, Cerner, EPIC, AllScript, SystemOne, WellSky and MedChart, to name but a few. However, it is also possible for platforms to link and integrate with medication wholesalers, finance systems and many more stakeholders, with a view of delivering a patient-centric supply chain.
The global challenge
The World Health Organisation recognised the severity of medication errors and more than 5 years ago, introduced a Global Patient Safety Challenge, Medication without Harm, with the ambition of reducing avoidable medication-related harm by 50 per cent. The scale of the issue within the UK is worrying; in 2018 the EEPRU report, Prevalence and Economic Burden of Medication Errors in the NHS in England, further highlighted the sheer scale of medication errors taking place.
The shock of these findings led to a review, which set the healthcare system on the path to technological solutions with the impressive adoption of the ePMA systems. According to a National Institute for Health Research (NIHR) funded study, high-risk medication errors can be reduced by up to 50 per cent with the implementation of this technology.
The next step; interoperability
Linking and integrating ePMA and EPR systems with complementary systems such as inventory management tracking systems, electronic controlled drug solutions, robotic dispensing systems and automated medication dispensing cabinets is the next step in truly driving down medication errors. NHS Trusts are now taking digitalisation a step further by investing in integrated electronic health record (EHR) systems.
EHRs represent a step beyond the standard patient medical history found in paper-based patient medical records and include a broader view, including information from all the clinicians involved in a patient’s care. Importantly, they also share information with other healthcare providers, such as laboratories and specialists. This approach enables NHS Trusts to enhance their operational and financial efficiencies and improve the experience for staff working at multiple sites.
Interoperability with partners helps ‘close the loop’ in the medication management process; not only does it enable optimisation of medication administration, it also provide a full access to patient data records allowing for complete visibility and accountability. For patients, it means healthcare professionals have up-to-date access to all information, irrespective of the treatment venue, enabling the delivery of high-quality, coordinated and informed care. Integration also allows for additional features and shared data with Omnicell pharmacy technology automation and intelligence solutions to drive inventory optimisation, diversion management, medication usage analytics, compliance and population health services.
A collaborative partnership approach
Omnicell prides itself on being a long-term partner to hospitals as a quality, trusting relationship supports a smooth transition to new, technology-enabled ways of working – supporting full buy-in and adoption by staff. Technology solution providers should spend time on-site, understanding different workflows in various departments and proving expert guidance on how adoption can best be used to make significant time and cost savings quickly. For example, the medication needs on an intensive care unit are different to the needs of an orthopaedic ward.
But what is the optimum solution for each of those wards, and which model of interoperable technology is going to be the most effective when it comes to achieving zero errors, zero waste and zero time-consuming process for staff? The future must therefore be one of sharing, co-operation and transparency; between systems, between patients and healthcare providers, between healthcare providers and industry experts and between different healthcare disciplines – all driven by knowledge and supported by data.
Conclusion
Interoperability solutions are a great opportunity for the healthcare sector and could be a crucial factor in realising the future of our much-loved national health service by presenting the sector with cost, safety and efficiency opportunities. With the right partners, Omnicell’s solutions can transform medication management and create synergies across healthcare enterprises. Technology doesn’t stand still and, looking to the future, interoperable technology solutions, data and AI have the power to change the healthcare landscape beyond recognition.
Chesterfield Royal Hospital introduced ward based automation systems for medicines to further reduce the risk of error and increase efficiency, with the ultimate goal of improving the management of medicines in the ward environment and reducing the burden placed on nurses and pharmacy staff. Martin Shepherd, Head of Medicines Management at Chesterfield Royal Hospital NHS Foundation Trust, commented: “This is a significantly better and safer way of dealing with ward medicines. The risk to patient safety is lower as we have reduced our dependence on manual processes. It provides a safety net, reduces the risk of products being wrongly selected and near misses. Integrating the ward-based systems with PMA only strengthens that level of security. It helps us in our drive to ensure that patients receive the right medicines at the right time.”
St Mary’s hospital already had a ward level electronic prescribing system in operation for two years when they decided to take the next step in patient safety and automation by installing Omnicell automated medication dispensing cabinets in all care areas. Jackie Harry, NICU Ward, Isle of Wight NHS Trust, commented; “We have much better stock control and expiry date management, and it’s really easy to use even in an emergency. We have saved time hunting for keys and searching in cupboards – we know we have the stock and the cabinet takes us to it. Invaluable. Really time efficient and safe.”
Ed Platt, UK Sales Director, Omnicell UK & Ireland
This article was kindly sponsored by Omnicell.
To learn more about the importance of interoperability, visit Omnicell.co.uk or email:
Finding the right support to provide the NHS with the capacity needed
By David Duffy
Dr Jean Challiner, Medical Director for Medinet, outlines how the NHS must harness spare capacity from all corners of the health and care sector to meet this period of unprecedented service demand.
As has been made abundantly clear by the Prime Minister earlier this month, the NHS is suffering from a severe capacity crisis. In addition to emergency departments tackling the toughest winter on record, 7.21 million people are currently on an elective care waiting list and staff shortages are crippling service delivery.
The Prime Minister himself acknowledged that these trends existed prior to Covid-19 but the pandemic has escalated the problem beyond what the NHS is able to tackle without added support. “With so many people waiting longer and longer for elective care, patients’ conditions are worsening and becoming urgent for some,” reflects Dr Jean Challiner, Medical Director for independent healthcare provider, Medinet.
Dr Challiner stresses that for Medinet, who have a two decade history of providing dedicated ‘insourcing’ for NHS trusts to boost capacity, the time patients are spending waiting for treatment is having a drastic impact on their work. “We used to almost exclusively offer capacity in the NHS for low complexity day cases, but now the priorities within the NHS are very different, and there is a growing need for us to address more urgent and more complex cases.”
Medinet holds the country’s largest pool of expert clinicians across 20 different specialties, and supplies teams to provide additional clinical capacity to enable hospitals to meet waiting times targets and then work with them to ensure these are not breached. In the last 12 months, 170,000 patients have been seen and treated by Medinet’s clinical teams.
The fact that Medinet teams work in close conjunction with NHS clinical teams and within existing estates means that they can adapt their service offering to include more complex surgery when needed. This includes cancer surgery and other procedures that fall under the realm of specialised commissioning. Medinet’s large pool of consultants, often made up of part-time NHS doctors or recent retirees, can perform most procedures, although they rarely tackle acute emergency procedures.
Reforming the referral process
Beyond directly boosting capacity with additional staff, Medinet have looked to enhance NHS efficiency and bring down backlog figures by reducing time to referral for patients. With cataract surgery, (accounting for one of the largest elements of the elective waiting list with 600,000 patients waiting for a procedure) patients are now having to wait up to two years to have their cataracts assessed.
“We are seeing some trusts getting twice as many referrals in certain areas as before and you can’t instantly train the necessary staff to meet this demand in the short term,” says Dr Challiner. “Part of our process is to not only bring in additional direct expert capacity where required but also help enhance overall efficiency or perhaps deploy existing resource differently.”
Based on a study conducted with a customer in Scotland, Medinet consultants have recently put forward recommendations to bring down cataract wait times across England, particularly for low risk patients. The study set out to determine the suitability of community cataract referrals for a one-stop cataract surgery service and the target areas for referral refinement. The results of the study showed that waiting time was significantly reduced – an average of 30 weeks for one-stop patients. Approximately one quarter of referrals were considered suitable for the one-stop service and many more may have been suitable if there had been more information in their referrals.
Capitalising on system reform
While Medinet services are still primarily commissioned by individual NHS trusts, the development of integrated care and closer collaboration between individual providers could potentially create opportunities for Medinet to expand its service offering elsewhere. “There is a huge opportunity within ICSs to change the model of harnessing spare capacity and applying [it] to other parts of the system. ICSs must provide the framework for providers to break out of regional, professional and organisational silos and boundaries to alleviate the capacity crisis currently being faced by the NHS.
“As providers evolve their service offerings to meet new challenges, they must be able to highlight where new capacity where is required without fear of reprimand.”
Encouraging active dialogue
Under no illusions, Dr Challiner acknowledges that the Medinet model is not a magic bullet to NHS capacity pressures as there are fundamental obstacles that can restrict impact. “Operating within existing NHS estate allows us to work much closer with NHS teams,” she says, “but we face regular challenges with bed availability, as we cannot conduct day case surgery unless there are beds available for recovery if needed. We also often have difficulty in simply finding the space within a trust for Medinet to operate in work or having a trust staff lead on hand to provide trouble shooting assistance or can locate replacement equipment if required.
“We encourage trusts to highlight new ways in which we can boost capacity. We are seeing an NHS that is working tremendously hard, and we want to help them. Nothing is off bounds for us, to help tackle what is most important, so we need the NHS to talk to us, and engage in discussions to look for possible solutions that are risk assessed and will work.”
Medinet’s position as a capacity booster has placed it in a unique position to reflect on the various challenges that lie within the NHS backlog. Last year, the organisation released its Manifesto for Better, outlining how they plan on supporting hospitals across the country to support commitments to improve access to treatment, empower patient choice, and provide the capacity required in response to the growing backlog of elective services.