The 10-Year Health Plan: A win for community pharmacy?
By Samantha Semmeling
The government’s 10-Year Health Plan outlines a major shift in NHS priorities, aiming to move care closer to communities, emphasise prevention, and harness digital tools. Central to this vision is an expanded role for community pharmacy, raising questions about how the sector will adapt and whether it is equipped to meet these ambitions.
The government’s 10-Year Health Plan sets out an ambitious transformation for the NHS underpinned by three major shifts: hospital to community, analogue to digital, and sickness to prevention. At the heart of this transformation is the proposed development of a ‘Neighbourhood Health Service’, where pharmacy is set to play a vital role.
The plan outlines a clear transition for community pharmacy, from a predominantly dispensing to a more clinical, preventative and digitally-enabled role. Over the next five years, the government proposes that community pharmacies will:
Manage long-term conditions such as obesity, high blood pressure and high cholesterol
Deliver more preventative services, including vaccinations and screening for cardiovascular disease and diabetes
Support complex medication regimes and offer independent prescribing
Be linked into the Single Patient Record, enabling more seamless service delivery
These proposals build on the success of existing services like Pharmacy First and hypertension case-finding, both of which demonstrate the value of pharmacy in improving access and early intervention. However, this success hinged on public awareness, strong pharmacy leadership, and swift IT integration – which must be central strategies if ambitions for the sector are to be realised.
Pharmacies are critical for prevention as they are well-embedded in local communities, but particularly so in underserved areas that often face the highest burden of chronic disease. However, pharmacies must be equipped with the right tools and training. Innovative diagnostic technologies, such as point-of-care testing, can support early detection and intervention. Although there have been some promising pilots, they are not yet used at scale. Deploying such tools in tandem with workforce training will be essential to delivering preventative services in community pharmacies.
Public Policy Projects (PPP) has previously advocated for a more integrated role for community pharmacy, parity across primary care and a broader understanding of the sector’s role beyond clinical services and medicines optimisation.
Community pharmacies are hyper-local, highly trusted and universally accessible, offering huge potential to deliver social value. From providing culturally sensitive health advice, supporting marginalised populations, or acting as an informal hub for wellbeing, community pharmacies are ideal settings to form part of the emerging Neighbourhood Health Service.
However, unlike general practice, community pharmacies do not hold registered patient lists and often serve individuals who move across geographical boundaries. As such, new services must be designed around the needs of patients, not tied to artificial catchment areas. Primary care contracts which are complementary and integrated by nature, allowing providers to collaborate, not compete, will be essential to seamless service delivery.
The 10-Year Health Plan marks a pivotal moment for community pharmacy. It recognises many of the sector’s often overlooked strengths and proposes a more strategic role for pharmacies in health and care delivery. However, these opportunities must be matched with sustainable funding, contractual reform, and meaningful collaboration across all system partners.
SAR pressures on the NHS: Why automation is now critical
By Sara Yirrell
Subject Access Requests (SARs) are rising sharply across the NHS, placing increasing strain on trusts. With mounting regulatory pressure and limited resources, Bradford District Care NHS Foundation Trust has taken action, introducing automation to ensure timely responses and protect sensitive patient data.
The number of Subject Access Requests (SARs) being submitted to the NHS is mushrooming year-on-year, and if trusts are left to manage with their current technology set up, many run the risk of falling behind the one-month deadline to complete each request and falling foul of regulations because they have neither the time, nor capacity to keep up with demand.
With the NHS 10-Year Plan also now published, aimed at modernising the health service in England and ensuring it is fit for purpose, decisions must be made on how to streamline core processes and make the whole experience better for not only people working within the NHS, but crucially, the people using it: the patients.
Regulatory requirements such as the UK GDPR and the Data Protection Act 2018 are growing in complexity, and healthcare organisations need robust systems in place to protect sensitive data, and help them respond quickly and efficiently to demands.
Case study: Bradford District Care NHS Foundation Trust
Bradford District Care NHS Foundation Trust is seeing the number of SARs increase by around 100 a year, and has currently received around 700 requests in so far 2025.
Sarah Briggs, Data Protection Manager at the Trust, explains that the SARs were from mixed sources and varied, including from the patients themselves; a solicitor acting on their behalf; police officers that are carrying out investigations; or councils that might be looking into protection orders. They also come from regulatory bodies looking at the Trust’s fitness to practice within the NHS.
She says the Trust had seen an increase in people exercising other rights as well, such as the right to rectification, having things amended or removed completely, and reporting that their records have been accessed inappropriately.
The matter has been exacerbated by the inclusion of emails and email trails, which increases the number of documents needing attention, she added.
Drowning in administration
Briggs said the sheer number of SARs was beginning to weigh the team down and cause sleepless nights.
“The sheer volume of SARs and the different challenges for different types of requests is our biggest challenge,” she says. “We’re a mental health Trust, so some of the records we have on patients with a long history of mental health issues can mean their records are huge. The problems start with struggling to get the records out of the system due to the size of the file which crashed the systems.”
Briggs says the more requests that came in, the more the team were stretched, and the harder it became to hit deadlines.
“You’re not on top of your targets or your workload, and it is really flattening for people not being able to feel like they were doing a good job. As the requests increased, we were not able to spend the time we wanted and it often felt like we were just firefighting,” Briggs adds.
Finding a better alternative
It was the above challenges, and the need for a new approach to SARs, that spurred the Trust to start looking into alternative technology
Briggs says that when she and her team started using Smartbox.ai technology, the functionality it added helped to reduce stress among her team almost immediately.
“The fact Smartbox.ai could handle emails was a massive thing. As was one of the functions – de-threading – which meant we could get rid of duplicates and identify chains of emails,” she says. “It also meant we didn’t have to import Exchange files into our own Outlook, meaning that multiple people could be working on a SAR at the same time which helps to save time and allows us to swap and change tasks when we need to.”
Briggs says that one example of a SAR she received involved 19,000 emails, but by using Smartbox.ai’s technology to remove duplicates, it reduced the number down to a ‘more manageable’ 1,800 files.
“It made such a difference about my own approach to a task and made you feel better about doing it,” Briggs emphasises. “We can also split documents into manageable chunks with Smartbox, rather than feeling overwhelmed.”
Another feature that was a game-changer – the Dictionary function – allows users to create lists of words or ‘risk indicators’ that need to be removed/redacted and implement them immediately.
“With mental health records there is a lot of content in there and sensitive words such as suicide, assault, termination,” explains Briggs. “This tool will help us ensure we don’t miss anything that could cause somebody harm and distress.”
She added that the option to use different colour redaction highlighters was a useful function which made it easier to explain away the information underneath should questions arise.
Communication is key
Another key positive about working with Smartbox.ai is its willingness to listen to feedback and act on it, Briggs claims.
For example, when her Trust first started using the technology, redactions were in black, but Bradford District Care NHS Foundation Trust always redacts information in white, which could have been a serious issue. But after a consultation with Smartbox.ai, the Trust’s needs were taken into account, and that functionality was built into their version of the software.
Simply by listening to its customer needs and acting on it, Smartbox.ai made a big impact, Briggs concludes, leaving her happy to recommend the technology to other Trusts.
“If you are working with technology like Smartbox.ai that is more intuitive and is keeping up with and adapting to how you need to work, it is easier for us to bring on new staff to train and it is easier for them to learn. I would say it is worth other Trusts, particularly Mental Health Trusts, looking into Smartbox.ai.”
If you need help streamlining your SAR processes and are drowning in administrative paperwork, get in touch with Smartbox.ai today and see how we can help you.
New report launched to improve productivity measurement in healthcare
By Integrated Care Journal
The report calls on the NHS to adopt multi-faceted measures that better reflect long-term investment, patient outcomes and workforce resilience, alongside greater evaluative and technical integration to bridge the gap between local insights and national decision-making.
A new technical report on Measuring Productivity in Health Care has been published by NHS Arden & GEM Commissioning Support Unit (CSU). Commissioned by the Health Foundation, the report provides an in-depth examination of how productivity in the NHS is currently assessed and how it should evolve to meet the growing challenges facing the health system.
Set against a backdrop of increasing demand, constrained resources and post-pandemic recovery, the report looks at how we measure, and how we should measure productivity in such a complex system as the NHS.
Katie Fozzard, Senior Economist at the Health Foundation, said: “The government has placed significant emphasis on increasing NHS productivity – setting a stretching target for the health service to deliver 2 per cent annual productivity growth. The way productivity is measured, and whether it captures what matters most, is therefore of crucial importance. This report is a vital resource to help us understand the different ways that productivity is measured and areas for improvement.”
Drawing on a wide body of literature and engagement with stakeholders across government, academia, NHS England and local health systems, the report explores the current strengths and limitations of existing productivity metrics, also looking forward to recent developments in productivity measurement, as set out in the ONS recent Public Services Productivity Review. It highlights persistent challenges such as fragmented data, inconsistent coverage across settings, and a lack of tools to evaluate long-term investment, preventative care and workforce resilience.
Rose Taylor, Executive Director Health and Care Transformation at Arden & GEM said: “Understanding and improving NHS productivity is essential to delivering high-quality care with finite resources. This report provides a fresh lens on how we measure productivity in such a complex system, highlighting where current metrics fall short and where new approaches can drive meaningful change.”
The report highlights the breadth of reasons for measuring health care productivity and corresponding approaches. It proposes a new classification framework to better align metrics with their intended use, whether for system-level planning, local service improvement, evaluating resource allocation or national financial accountability.
Among its key areas for development, the report calls for:
The adoption of multi-faceted measures that better reflect long-term investment, patient outcomes and workforce resilience, to strengthen how measures align with future service needs
Greater integration of micro-level evaluative and macro-level technical approaches to bridge the gap between local insights and national decision-making
Investment in metrics that account for the value of preventative care beyond short-term costs
Improved tools to measure productivity across evolving care pathways and system partners, including social care and the independent sector
The Health Foundation will build on these findings in future work to support better long-term decision making across health and social care.
The full Measuring Productivity in Health Care report is available here.
NHS long-term plan, in the short-term: Where tech must help now.
By Dr Mark Ratnarajah
Strategic realignment over the next 10 years is important. But what are the practical, inarguable early wins the government must try to achieve for an NHS now? Dr Mark Ratnarajah, UK Managing Director of C2-Ai and practising NHS paediatrician, offers some answers.
As the unveiling of the long-awaited NHS 10-Year Health Plan rapidly approaches, the need for certainty and direction has never been more pressing.
Staff at the centre are already being reorganised, systems are being re-defined, and productivity and workforce pressures facing the frontline mean that new ways of solving pervasive problems are all but guaranteed to be heralded as the plan hits the shelves.
The Chancellor’s June spending review has earmarked £10bn for digital – but looking beyond the NHS App and a new single patient record, how might this money be used to respond to pressures with new care models, and what must be done much more immediately rather than over the decade?
Here’s seven priorities the new long-term plan must address in the short-term.
Managing electives, preventing demand escalation
A key election pledge, the elective backlog will undoubtedly be prominent in the plan. Though important progress has been observed, NHS Confederation’s recent annual conference reminded delegates that millions of people are still on waiting lists. Addressing the real problem is however more complex than counting numbers.
The underpinning matter is how to manage demand and serve those in greatest need when they need it, so that they don’t deteriorate and subsequently compound demand growth. That’s a complex question but it is possible to answer by a shift in thinking: one where systems respond to a complete individual’s risks and consider the wider human impact, so that we don’t just shift demand from outpatients to A&E or primary care, and inadvertently push patients into other costly parts of the health system.
An immediate opportunity is to learn from pioneers, who have put technology to good use in identifying patients at risk of harm or added complexity while waiting. Trusts and systems have responded with interventions in the community to prevent downstream escalations. In those examples entire patient cohorts have been better supported, and have shown reduced emergency attendances, complications, and lengths of stay.
The plan’s response must be about more than keeping things hanging together. It must be about supporting the customer: the patient; especially if the NHS is to manage an anticipated overall 40 per cent growth in demand in the next 10 years – suggested by compound growth metrics being observed.
Driving prevention, anticipatory health, new citizen responsibilities
Prevention too has sat on healthcare conference agendas for decades. Now it must become reality. In part that means surfacing hidden risks, targeting interventions in communities to avoid harm, and looking beyond boundaries: enabling collaborative data insights on risk across NHS and local government.
New anticipatory pathways are what this really means in practice: predicting health needs at the earliest point. Proactive, rather than passive, healthcare means reducing reliance on the reactive and ensuring fewer patients coming through the front door. We need to address individuals’ needs at-scale before they manifest themselves in expensive ways that are not optimal for the patient or system.
Giving patients agency with targeted data is a must so they are participants and empowered to direct their own health decisions; and to ensure better readiness for the inevitable encounters such as surgery.
As citizens we need to take more responsibility. In mental health services patients are sometimes asked to commit to a contract that includes their responsibility. We might see more of that in managing more long-term conditions. That can only work if we can understand what specifically we expect patients to do to make a difference – technology-driven insight can make that relevant for each patient’s risks. We might better alert patients to the community activities that can help them, and we might better ensure the provision of those facilities to move from medicalisation to a wellness and wellbeing focus.
Supporting the new ICS landscape to manage local demand
Organisations designed by nature to enable cross-organisation convergence around patients, integrated care boards are seeing systemic overhaul just a few years after their creation.
As budgets and headcount are cut, and ICS consolidation advances, they could benefit from technology more than ever in gaining the insights to understand local needs and organise health and social care service configurations.
These organisations will remain central in enabling care to move closer to communities and in preventing downstream cost and pressure. Technology suppliers must support them during a turbulent time so that they can evidence decisions on where and how to deploy resource to address wider determinants of ill health, to respond to citizens and not just patient needs, and to avoid a refocus back on acute care.
Delivering the digital and data revolution
Digital to analogue is something that must now succeed to enable integrated care and decision-making.
New and innovative ideas must be able to scale where they show impact. And we must make a success where commitment has been made. Politics aside, imagine the conversations we could have been having about digital, rather than a focus on moving away from paper, if the National Programme for IT had actually succeeded.
We now need to focus on turning insight into action, on building optimised pathways of care, and on how we can make better decisions with amenable and accessible data that can change practice.
Improving maternity and peri-natal safety
Not in itself one of the three shifts, but maternity safety continues to hit headlines. The ability to deliver safe care here is the barometer for the health service. Well mothers and babies must expect to go in healthy and come out healthy. If we fail that, then we have a key confidence issue for the wider NHS.
Equally, if we can get maternity right, then we can probably get everything else right. In the short term the plan has an opportunity to bring about renewed transparency in quality and safety. That means more than investigations and reports that only shed light on matters after they have become scandals. It also means doing more than measuring compliance with processes through audit.
At least some of the billions being used for technology could be turned to address and prevent avoidable harm in maternity through data-driven insight, that allows early identification of service and system-level problems. There is an opportunity to create new intelligence, but only if we embrace a learning culture.
Building a learning, safe NHS
The fact that safety scandals continue to emerge shows there is more to do to ensure a culture of learning in the health service. Just as real-time insights could prevent harm happening for maternity, the same is true for other services across health and care. Reliance on reports that take place once every few years is not enough. A culture of ongoing transparency, where we can be open about mistakes, must be the direction of travel.
Some of the best performing hospitals in the world are already doing this. Karolinska University Hospital in Sweden, for example, delivers some of the best survival and complication outcomes in the world for severely injured and unwell patients. It has used UK grown technology to prove this, and in a relentless pursuit of quality, continuously works to understand and act on any sub-optimal outcomes. Such approaches could be equally impactful in the UK to allow us to both celebrate excellence and deliver support where it is needed most.
Health equals wealth, and vice versa?
There was a reassuring investment in health in the spending review. But with cuts to other government departments, and the need to respond to ever rising global insecurity, public spending is under closer scrutiny than ever.
To deliver best value, the coming plan might therefore ask: what must we stop doing in order to fund new models of care delivery.
It might also ask questions about the relevance of industries that sit around the NHS to GDP – notably health tech, pharma and life sciences. Could the globally competitive nature of these UK companies be of interest as a means of wealth generation for the country, and to ensure it can continue to afford a health service?
And with phrases like ‘wealth is health, and health is wealth’ being increasingly heard, the plan might consider how a thriving SME sector that invests in the communities it serves could be a positive source for tackling inequity that so often leads to costly ill-health – wealth being a driver of health, and indeed the resilience of the nation.
Dr Mark Ratnarajah, Managing Director, C2-Ai and practising NHS paediatrician
Government promises clinical trials boost ahead of 10-Year Plan announcement
By Integrated Care Journal
The government is pledging to increase access to clinical trials for millions under its Plan for Change, which will eventually see NHS App notify users of clinical trials based on their health data and interests.
The government has pledged to increase access to clinical trials for millions as part of its drive to modernise patient care in the NHS and drive economic growth. The Plan for Change, set to be released as part of the upcoming 10-Year Health Plan, will enable NHS App users to browse and find trials suited their needs and interests, via the NIHR Be Part of Research service on the App.
The plan also aims to increase access to new treatments by accelerating trial set-up times and turning the UK into a ‘hotbed of innovation’. Through the App, public reporting will show which NHS trusts are delivering on trials and which area falling behind, with future funding set to be prioritised for the best performing trusts.
Eventually the plan will see the NHS App automatically match patients with studies based on their own health data and interests, sending push notifications to users’ phone about relevant new trials to sign up to.
It comes as the National Institute for Health and Care Research (NIHR) launches a UK-wide recruitment drive for clinical trials – the biggest ever health research campaign – to get as many people involved in research as possible. Adults across the UK are being urged to register, with underrepresented groups including young people, Black people and people of South Asian heritage particularly encouraged to sign up, at bepartofresearch.uk.
The 10-Year Health Plan will aim to bring transparency over which NHS trusts are performing well in clinical trials, and which are not. All NHS trusts and organisations will need to submit data on the number of trials being conducted and the amount of progress being made.
Public reporting will show the number of trials sponsored by both commercial and non-commercial sponsors at specific trusts and other organisations, including universities or primary care sites. It will reveal to the government, patients, investors, and Trust boards which NHS organisations are performing well and which are falling behind. Government investment will only be prioritised for the Trusts that can prove they can support the NHS to deliver the treatments of tomorrow.
Health and Social Care Secretary, Wes Streeting, said: “The UK has been at the forefront of scientific and medical discovery throughout our history. Some country will lead the charge in the emerging revolution in life sciences, and why shouldn’t it be Britain?
“The 10-Year plan for health will marry the genius of our country’s leading scientific minds, with the care and compassion of our health service, to put NHS patients at the front of the queue for new cutting-edge treatments.”
In recent years, the UK has fallen behind as a global destination for these trials, with patients and the wider economy missing out. It takes around 100 days to set up a trial in Spain, but around 250 days in the NHS. The plan will see commercial clinical trial set-up times fall to 150 days or less by March 2026 – this will be the most ambitious reduction in trial set-up times in British history.
The government is now pledging to cut set up times for clinical trials. Currently, trials have to agree separate contracts with each part of the NHS they want to be involved. The plan will introduce a national standardised contract which can save months of wasted time, as well as simplifying paperwork to remove duplication on technical assurances.
This means if any authority asks for evidence from a study, they can provide it once without having to spend time reframing that evidence differently to meet a separate criteria for another authority.
In the coming weeks, the government will publish its 10-Year Health Plan. The plan aims to restore the UK’s position as a world leader in clinical trials, enabling it to attract global talent and drive investment into the UK. The government hopes that this will spur economic growth, improve the standard of care to support a healthier population, and make the NHS more financially sustainable.
Professor Lucy Chappell, Chief Scientific Adviser at the Department of Health and Social Care (DHSC) and Chief Executive Officer of the NIHR said: “We know the benefits of embedding clinical research across the NHS and beyond. It leads to better care for patients, more opportunities for our workforce and provides a huge economic benefit for our health and care system. Integrated into the NHS App, the NIHR Be Part of Research service enables members of the public to be matched to vital trials, ensuring the best and latest treatments and care get to the NHS quicker.
“Ensuring all sites are consistently meeting the 150-day or less set-up time will bring us to the starting line, but together we aim to go further, faster to ensure the UK is a global destination for clinical research to improve the health and wealth of the nation.”
Dr Vin Diwakar, Clinical Transformation Director at NHS England, said: “The NHS App is transforming how people manage their healthcare, with new features letting them see their test results or check when prescriptions are ready to collect – all at the tap of a screen.
“We’re making it easier to sign up for clinical trials through the NHS App so patients can access new treatments and technologies earlier, improving their quality of care.
“The Medicines and Healthcare products Regulatory Agency (MHRA) – which makes sure that medicines and healthcare products available in the UK are safe and effective – has already improved its performance.”
Nicola Perrin, Chief Executive of the Association of Medical Research Charities, commented: “Clinical trials are good for patients, the NHS and the economy. But both commercial and non-commercial trials in the UK have closed because of failures to recruit.
“It’s encouraging to see the government recognise that boosting access to clinical trials must be a key part of the 10 Year Health Plan. Transforming clinical trials is an important step in truly embedding research in the NHS, securing the UK’s position as a leader in life sciences and offering a lifeline to patients.”
From diagnosis to remission: Delivering results at scale with T2DR
By Keren Miller
Diabetes and obesity cases in the UK are rising rapidly, putting increasing pressure on health and care services. But supported digital self-management tools are delivering measurable results, helping patients lose weight, increase physical activity, and in many cases, achieve remission, writes Keren Miller, Clinical Lead Dietitian for Diabetes and Diabetes Remission at Oviva.
Obesity and type 2 diabetes are among the most pressing health issues facing the UK. Today, around 12.5 million UK adults are estimates as living with obesity and more than 5.8 million with diabetes, numbers that are rising year-on-year. These conditions place a significant and growing burden on the NHS, both financially and in terms of long-term health outcomes. From heart disease to kidney failure, obesity-related complications are reducing quality of life and putting lives at risk.
A new way forward: evidence-based, digital-first care
We believe there’s a better way forward. As the obesity crisis escalates, scalable, evidence-based solutions are urgently needed, and digital programmes can play a crucial role. Oviva provides specialist digital type 2 diabetes and weight management programmes. Our mission is to empower people to make sustainable lifestyle changes, creating a healthier future for those living with weight-related conditions by offering highly accessible and effective technology-enabled support.
Delivering results: The NHS T2DR Programme
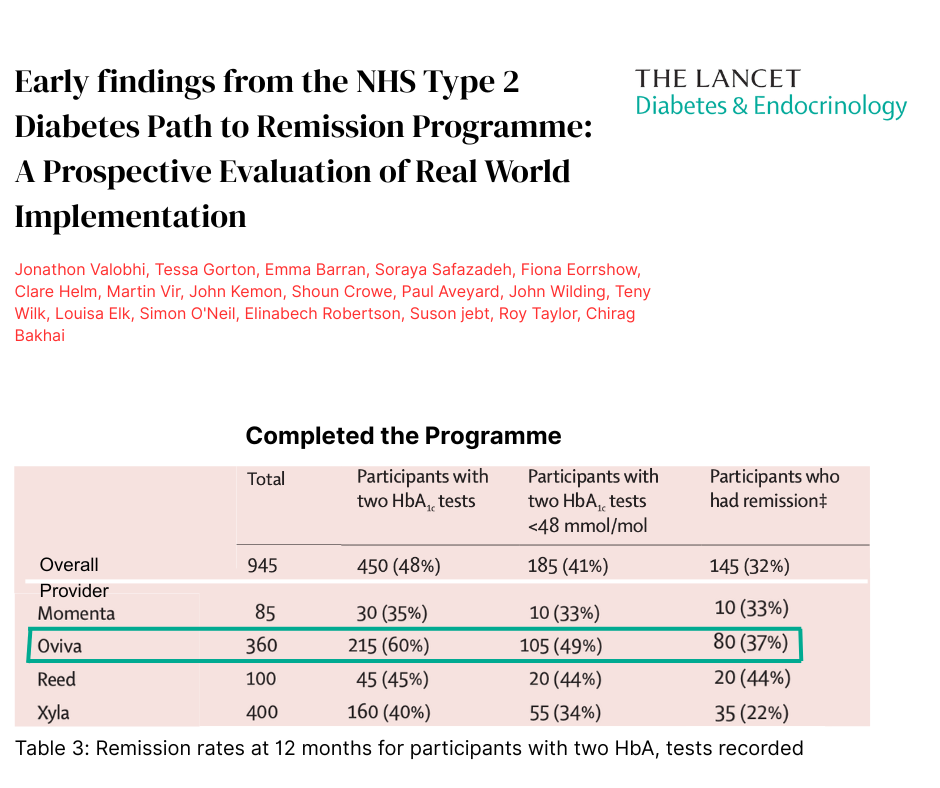
Through the NHS England Type 2 Diabetes Path to Remission Programme (T2DR), Oviva is supporting people living with diabetes to lose weight, reduce their need for medication and improve both their blood pressure and blood glucose levels.
An NHS assessment published in The Lancet showed that “remission of type 2 diabetes is possible outside of research settings, through at-scale service delivery”.
Oviva was proud to feature as a lead provider, delivering strong outcomes reporting:
8.7 per cent average weight loss for patients
37 per cent of patients who completed the programme achieved remission status
18 per cent of patients lost at least 15 per cent baseline weight
This real-world evidence confirms that digital T2DR programmes can be an effective, scalable solution for people living with type 2 diabetes.
As the NHS continues to evolve in response to rising obesity and diabetes rates, it’s clear that effective, scalable solutions like NHSE’s T2DR programme are more important than ever. The results of the T2DR programme show that real change is possible, not just in research trials, but across the country.
Oviva is proud to support the NHS with programmes that work. Our digital model removes barriers to access, reaches underserved communities, and empowers people to take action in a way that feels achievable and sustainable.
Paul’s story: Transforming health, one step at a time
Paul, 59, from North London, was stunned to learn he had been diagnosed with type 2 diabetes and a heart condition – a wake-up call that inspired him to take action.
Like many, Paul’s weight had crept up during the Covid pandemic, made worse by a sedentary desk job. Determined to make a change, he joined the NHS T2DR programme and embraced the opportunity to transform his health.
Paul admitted the total diet replacement phase was challenging, but his perseverance and discipline paid off. Supported by Oviva coaches, Paul committed to the programme and saw incredible results. Even two months after completing the programme, he continues to use the Oviva App to track his progress and access learning content, keeping his motivation high.
Paul, 59, lost 50kg after 14 months on the T2DR Programme
After just 14 months, Paul’s progress has been remarkable:
Weight loss: 50kg, now maintaining a healthy weight of around 92kg
BMI: Reduced from 47 to 29 kg/m²
HbA1c: Improved from 81 mmol/mol to 38 mmol/mol, well into the target range
Activity: Paul is walking at least an hour a day, adjusted cardio due to his heart condition
Paul’s story is a testament to the transformative power of the T2DR programme, and a reminder that, with the right support, patients can take control of their health and reverse type 2 diabetes.
To find out more about how we’re empowering people to achieve lasting improvements in their health and wellbeing, visit oviva.com.
North West extends digital support for up to 275k unpaid carers
By Integrated Care Journal
The move sees Wigan Council join a growing number of local authorities aiming to better support unpaid carers through accessible, round-the-clock digital tools and resources.
Up to 275,000 unpaid carers living across the North West of England can now access an expanded range of support services, including an online community forum and tools to help claim financial support, as the region looks to boost help for this vital community.
This milestone comes as Wigan Council announces it has become the latest local authority in the North West to roll-out a tech-powered initiative designed to connect and support those looking after friends, family and neighbours. This support is being delivered in partnership with the UK’s largest community of unpaid carers, Mobilise.
This latest backing from Wigan Council takes the number of North West carers able to access the digital support to up to 275,000.
At least 31,442 people identify as unpaid carers in Wigan, comprising 1 in 10 of the local population. The new initiative will provide an added layer of on-demand support for anyone who looks after someone in the area, including those who may not identify as ‘carers’ or realise they are entitled to support.
As part of this, the initiative aims to uncover and widen access to support for 3,900 people who have not previously engaged with any support in Wigan.
Wigan Council follows nine local authorities in Cheshire and Merseyside who joined the same initiative in October last year. This saw 243,000 unpaid carers in Cheshire and Merseyside gain access to the tech-powered support. 8 in 10 (79 per cent) Cheshire and Merseyside carers had not accessed any support prior to the digital initiative rolling out across the region.
The new services can be accessed remotely via an online hub and include:
An online peer community of hundreds of thousands of fellow carers from across the UK, with a community forum and regular events to share experiences and advice
Self-service tools to help carers understand the different benefits they may be entitled to (including Carer’s Allowance), check their eligibility, and access different support
Tailored support guides on everything from how to balance caring with full-time work, to managing personal health and wellbeing while looking after someone else
Information on carers’ rights and relevant social care law, in line with the latest government guidance
An AI-powered ‘Mobilise Assistant’ is also available to help carers quickly and easily find the specific information, resources or support that they need, using their own words.
In Cheshire and Merseyside, the majority (51 per cent) of carers currently accessing these digital services rely on the support outside of working hours. Now also available to carers living in Wigan, the on-demand offering will supplement existing support in the region, including in-person services provided by local organisations such as the Wigan & Leigh Carers Centre.
Councillor Angela Coleman the Cabinet Member for Adult Social Services at Liverpool City Council, commented: “Our priority is ensuring that all carers living in Liverpool can access the support they need, when they need it. Partnering with Mobilise to offer on-demand, remotely available services have helped extend our ability to deliver this support. With more carers engaging with support for the first time, and the majority accessing the new services outside of working hours, the impact is already clear to see.”
The initiative in both Wigan and Cheshire and Merseyside is being funded by the Government’s Accelerating Reform Fund.
For more information about the support now available in Wigan, see here. For more information about the support available across Cheshire and Merseyside, see here. To start accessing support today, the Mobilise app can be downloaded via the Apple App Store or Google Play, with more information available on Mobilise’s website.
Case study 1:
Alison and her husband
Alison Lodder, who cares for her husband in the North West, said: “My husband was diagnosed with MS almost thirty years ago, just two years after we got married. I’ve cared for him ever since. During my caring journey, I’ve found different forms of support have helped at different times. For example, my local carers centre has been a lifeline in the past, and a care worker now comes to the house to provide more regular support whilst I get ready for work in the mornings. Juggling part-time work with my caring role restricts the times that I can access wider support. But, since joining Mobilise, I’ve always had another carer to chat to when I find a moment for myself in the evenings, or an expert on hand to offer advice when I need it the most.”
Suzanne Bourne, co-founder and Head of Carer Support at Mobilise, commented: “As unpaid carers, it’s vital we get the support we need to protect our own wellbeing, and continue to look after our friends or family at the same time. But caring responsibilities don’t always start and stop in line with traditional working hours, or allow us to leave those in our care alone. This is where on-demand digital support can help.
“I’m grateful that, alongside local carers organisations like Wigan and Leigh Carers Centre, Mobilise is now able to help more carers across the North West access support whenever and wherever they need it. Our new partnership with Wigan Council, and our continued work with local authorities across Cheshire and Merseyside, will help ensure that no one has to navigate the daily realities of caring alone.”
Case study 2:
George, who cared for his mother in the North West
George Smith who cared for his mother and lives in Cheshire, said: “I moved in with my mum in 2023 after a nasty fall led to mobility issues and various complications that left her unable to look after herself.
“You don’t expect to become a carer. I certainly wasn’t prepared for how it would impact me physically and mentally. There were many times when I felt lonely, guilty, and like I was losing my sense of identity. Talking to other carers helped me realise it was okay to take time out for myself. The Mobilise community also helped me realise I wasn’t alone. They opened my eyes to how many of us look after loved ones who we might once have relied on ourselves, and how many of us will come to rely on those around us in future.
“I cared for my mum up until she passed away earlier this year. And I wouldn’t have had it any other way.”
Councillor Keith Cunliffe, Portfolio Holder for Adult Social Care at Wigan Council, said: “We are proud to be working with Mobilise alongside Wigan and Leigh Carers Centre in this innovative partnership to better support unpaid carers across Wigan Borough. Unpaid carers are vital to our communities and it is so important that we continue to find new and effective ways to support them. By embracing digital innovation, we are ensuring carers can access the help they need, when they need it and in a way that fits around their busy lives.”
Christine Aspin, Chief Officer at Wigan and Leigh Carers Centre, said: “As Chief Officer at Wigan and Leigh Carers Centre, I am announcing our partnership with Mobilise. This collaboration alongside our ongoing work with Wigan Council will enable better support for unpaid carers in the Wigan Borough. By utilising innovation and technology, we aim to address carers’ needs effectively, providing essential resources, support, and assistance at a time and convenience suitable for the carers.
“This partnership emphasises the importance of collective efforts in fostering positive community engagement and improving wellbeing. We aim to offer support beyond conventional hours, ensuring targeted assistance for working carers and those who cannot access daytime services. Caring does not fit a 9-5 model, so support will be available to carers as and when needed. Our goal is to ensure that every carer in our community has access to the help they need, precisely when they need it most.”
Royal Pharmaceutical Society unveils Greener Pharmacy Toolkit
By Integrated Care Journal
The new RPS Greener Pharmacy Toolkit provides prompts to introduce more sustainable practices to reduce emissions, improve patient care, prevent ill health, tackle medicines waste and achieve efficiency savings.
A new digital self-assessment tool, designed to help community and hospital pharmacy teams take practical action to reduce the climate impact of pharmacy services, pharmaceutical care and medicines, has gone live.
The Royal Pharmaceutical Society’s (RPS) Greener Pharmacy Toolkit outlines three levels of accreditation – bronze, silver and gold – based on various actions that pharmacy staff can voluntarily take to make their pharmacies more sustainable, while supporting patient care. Achieving the target accreditation triggers a certificate, which can be displayed to demonstrate the pharmacy’s commitment to environmental sustainability.
Commissioned by NHS England and supported by Greener NHS, the Toolkit is free and open access, available for use by hospital and community pharmacy teams throughout Great Britain. The digital toolkit and accompanying guidance align closely with RPS’ work on sustainability which recognises the impact of climate change on health.
Minna Eii, RPS lead on the Greener Pharmacy Toolkit, acute medicine Advanced Pharmacist Practitioner and co-Founder of Pharmacy Declares, commented: “This pioneering resource is the first-ever toolkit to help pharmacy teams reduce their carbon footprint and a real step forward in using technology to improve practice and patient care. It’s backed by a wealth of expertise and the stages of accreditation make it the ideal starting point for those who want to reduce their environmental impacts but don’t know where to start, as well as driving improvements for teams already on that journey.”
President of the Royal Pharmaceutical Society Professor Claire Anderson, said: “Medicines account for 25 per cent of carbon emissions within the NHS so doing nothing is not an option. This free to access and easy to use toolkit will help hospital and community pharmacies across the country to promote sustainable practice and reduce their environmental impact. It’s another step in our strong commitment to enabling more sustainable pharmacy services.”
Community pharmacist Mrs Patricia Ojo, from Stevens Pharmacy, said: “Our pharmacy is an early adopter of the Greener Pharmacy Toolkit, progressing through the bronze level. We’ve appointed a sustainability lead and completed all clinical practice, people, operations, and strategy bronze descriptors. We’re halfway to attaining bronze and proud that much of what we are doing already helps to combat climate change. It’s great for the team to see how actions like teaching correct inhaler use and encouraging repeat dispensing contribute to better patient care and environmental sustainability. Despite being busy, we’re keen to continue making progress with the toolkit.”
Laura Stevenson, Associate Chief Pharmacist and Medicines Sustainability Lead at King’s College Hospital, London said: “At King’s we are delighted there is now a dedicated Greener Pharmacy Toolkit for hospital pharmacy. We can now engage our pharmacy teams with clear, practical guidance on sustainability; the toolkit supports teams in making informed decisions that promote a greener, more responsible pharmacy service. It will now be easier for pharmacy teams to play their role to combat climate change and we’ll be exploring how this can support our environmental sustainability efforts and make a real difference in our hospital’s journey to net zero. Together we can make pharmacy greener and more resilient for the future.”
The project was led by healthcare professionals with expertise in environmental sustainability and involved multi-stakeholder engagement and feedback. The RPS Greener Pharmacy Guide scoping review underpins the development of the toolkit, using an evidence-based approach to offer insights into its rationale, content, and structure.
Community care critical for improving diabetes outcomes: ICB diabetes lead
By Navodi Kuruppu
Dr Naomi Chinn, Clinical Diabetes Lead at NHS Humber and North Yorkshire ICB, sat down with PPP to discuss her advocacy of community-based diabetes care, its positive impact on both patients and the workforce, and the role of integrated neighbourhood teams, collaboration and networking.
2025 has ushered in a seismic shift across the UK health and care landscape. The abolition of NHS England is resetting the shape of health and care for the coming years. Integrated care boards (ICBs) are under increasing pressure following the mandate to cut costs by 50 per cent, anticipated mergers, and the publication of a new model ICB blueprint. Under this model, systems will be expected, among many other responsibilities, to commission new care pathways and services in support of the key strategic shifts outlined in the 10-Year Health Plan. The Plan, currently expected to be released at the beginning of July, is set to clarify several questions created by these reforms and how they will impact access and delivery of care, including diabetes.
Public Policy Projects (PPP) recently spoke to Dr Naomi Chinn, Clinical Diabetes Lead at Humber and North Yorkshire ICB. Dr Chinn, who took on her role in December 2024, has been working with her team on re-establishing the system’s diabetes work programme, and has long been an advocate for the strategic shift towards community-led care approaches.
Ahead of her appearance at PPP’s Diabetes Care Conference 2025, Dr Chinn shared some insights into current picture of community-led diabetes care within Humber and North Yorkshire.
With regards to this demography, Dr Chinn states that both patients and workforce would benefit from a shift towards community-led diabetes care. She believes that integrated neighbourhood teams (INTs) can provide vital support to staff across the system, ultimately optimising the quality of patient care delivered. This approach has already shown positive results through a prevention programme implemented in the region.
“The programme is delivered in local community centres and is supported by trusted community figures and attended by individuals living in the same neighbourhoods,” explains Dr Chinn. “Through this programme, we are holding annual diabetes reviews regularly and they are easily accessible at a nearby health centre, with retinal screening available in the room next door. Where needed, patients can be referred to specialist services such as podiatry, ultimately creating a joined-up, community-based care experience.”
Recently, the ICB has also introduced a programme of Local Enhanced Services (LES) for patients with type 2 diabetes, accessible through general practice. LESs are locally developed schemes designed to supplement core practice services, with variations in scope and funding across the country according to local need. This targeted investment is a result of the ICB’s recognition of the value of delivering better care closer to home, bringing both clinical and social benefits through this ‘left shift’ in care. An additional advantage is the potential to relieve pressure on secondary care services, allowing them to prioritise patients who require more specialised expertise and facilities.
“We know that both hospital and community teams are working harder than ever,” Dr Chinn adds, “so, this has to be about more than simply shifting patients and populations between settings; prevention must also be a core and continuous part of our service from the very beginning.”
The need for collaboration
As ongoing reforms ultimately aim to deliver a more integrated approach to care, collaboration with wider partners is key to make this vision a reality. Dr Chinn emphasises the value of working closely with ICS stakeholders, including primary care, secondary care and Voluntary, Community and Social Enterprise (VSCE) stakeholders, and the importance of engagement with patients.
An example of this collaborative approach is a recent design workshop led by Dr Chinn, which convened system partners to identify barriers to accessing diabetes care, share best practice and generate new ideas. Alongside this, Dr Chinn and her team launched a patient engagement questionnaire, asking patients who might be interested to participate in the work going forward. The feedback, combined with insights from recent GIRFT reviews for both adults and children and young people, has directly informed the development of the region’s diabetes work programme.
To support delivery and ongoing development, the team is establishing bimonthly advisory groups, in addition to a broader network meeting. This approach aligns closely with the ICB’s core principles and wider strategic initiatives, including recommendations from Lord Darzi’s Independent Review, to simplify and innovate care delivery at the neighbourhood level, re-engage staff, and re-empower patients.
“A problem shared is a problem halved”
Given the large population and geographical footprint it serves, Dr Chinn highlights that regional variation is one of the biggest challenges facing Humber and North Yorkshire.
“We are an ICB with a large geographical area and a highly diverse population,” Dr Chinn explains. “Achieving continuity across these regions, while also meeting local needs, is probably our biggest challenge. In some places, like Hull, we face one of the lowest GP-to-patient ratios in the country, which makes workforce development even more difficult.”
Despite these challenges, Dr Chinn acknowledges the importance of connection and collaboration in overcoming them, through the integration of workforce, patients, and partners and underpinned by prevention and local knowledge: “Bringing people together makes a real difference.”
Dr Chinn adds: “Sometimes it’s as simple as remembering that a problem shared is a problem halved. A challenge in Whitby today might be something Willerby overcame last year. Within the ICB, we are a small team, so building connections and keeping communication open, whether it’s asking for help or flagging concerns, is essential. Through networking, we’re starting to achieve this.”
As publication of the 10-Year Health Plan approaches, local systems like Humber and North Yorkshire ICB are already demonstrating the value of prevention and community-led care. Dr Chinn’s vision offers a scalable blueprint for a collaborative, community-led approach to diabetes care, that will be further discussed at PPP’s Diabetes Care Conference 2025 on Wednesday 25 June in London.
Holding our nerve: Making the ‘left shift’ a reality in health and care
By David Duffy
At a recent dinner hosted by Public Policy Projects and HealthPathways, senior NHS executives and leaders gathered to reflect on one of the most urgent challenges in health and care today: how to deliver a meaningful ‘left shift’ – moving care out of hospitals and into community settings, as outlined in the forthcoming 10-Year Health Plan. The conversation offered a candid look at the structural barriers that continue to impede progress, while also spotlighting the leadership, collaboration, and bold action required to overcome them.
The discussion was chaired by Len Richards, who stepped down as CEO of NHS Mid Yorkshire Teaching Trust in April 2025. With executive leadership experience in healthcare systems across both the UK and Australia, Richards has been a consistent advocate for integrated system working and for modernising health services through partnership-driven reform.
As Richards noted at the outset, much has changed in recent months. Financial pressures have deepened across the board, with providers and systems increasingly asked to deliver more with fewer resources. Meanwhile, major structural reform looms, including the anticipated merger of NHS England with the Department of Health and Social Care, and a sweeping review of the core functions of integrated care boards.
Despite these developments, many long-standing challenges remain unresolved. Hospital congestion and ever-growing waiting lists continue to plague the NHS, despite multiple central reorganisations. These pressures have fuelled a crisis in public confidence and severely undermined staff morale.
Drawing on his leadership experience in Australia, Wales, and the UK, Richards emphasised that real progress depends on genuine system-wide change. He highlighted his longstanding use of HealthPathways as a practical tool to support integration – a model that draws on clinical expertise, community knowledge, and patient experience. For Richards, HealthPathways’ system-wide approach to care pathway redesign has consistently delivered clarity, confidence, and hope during times of change.
This sentiment feels more poignant than ever, as the system now requires a whole-of-system approach to left shift – one that builds additional capacity, boosts productivity, and firmly places patients at the centre of care.
The reality of the left shift
Despite years of policy promises and widespread rhetorical backing, there was a shared acknowledgement that the shift towards community-based care has yet to take meaningful form. System leaders expressed frustration that, while the vision is widely accepted, progress on the ground remains slow. With funding still disproportionately directed toward hospitals, acute care continues to be treated as the default care setting, despite decades of political commitments to reallocate resources toward prevention and community services.
The message was unmistakable: the current approach is falling short – and in some cases, actively worsening outcomes for patients. Long waiting times, increasing health-related anxiety, and ongoing challenges in mental health services are eroding public trust. Transitioning to a community-based, preventive, and integrated model of care is no longer just an aspiration – it is fundamental to the sustainability of the NHS.
Yet, under the weight of existing system pressures, achieving this transformation feels increasingly out of reach. There was a strong call in the room for political rhetoric to be matched by bold, system-wide action, and for local leaders to be genuinely empowered to make decisions that reflect the needs of their communities.
A system that still thinks in silos
Despite years of policy promises and widespread rhetorical backing, there was a shared acknowledgement that the shift towards community-based care has yet to take meaningful form. System leaders expressed frustration that, while the vision is widely accepted, progress on the ground remains slow. With funding still disproportionately directed toward hospitals, acute care continues to be treated as the default care setting, despite decades of political commitments to reallocate resources toward prevention and community services.
The message was unmistakable: the current approach is falling short – and in some cases, actively worsening outcomes for patients. Long waiting times, increasing health-related anxiety, and ongoing challenges in mental health services are eroding public trust. Transitioning to a community-based, preventive, and integrated model of care is no longer just an aspiration – it is fundamental to the sustainability of the NHS.
Yet, under the weight of existing system pressures, achieving this transformation feels increasingly out of reach. There was a strong call in the room for political rhetoric to be matched by bold, system-wide action, and for local leaders to be genuinely empowered to make decisions that reflect the needs of their communities.
Leadership, risk, and public trust
Some leaders did highlight that large sections of the public still maintain that the hospital is the safest and most effective place within the sector to receive care. It is up to leaders, political and otherwise, to have a frank conversation with the public to address this trend and clearly articulate how health and care services can be accessed.
Leaders must be clear of purpose, instil confidence, and perhaps most importantly, hold their nerve in the face of political and institutional pressure. But bravery cannot stop at the hospital board room.
Several attendees emphasised the need for political courage at the national level. Without it, the system will remain risk-averse and locked into a cycle of short-term performance management at the expense of longer-term transformation.
There was strong consensus that DHSC needs to be brave in redistributing resources away from acute settings, even when these efforts run counter to entrenched assumptions or public sentiment.
Rebuilding public trust is paramount, and confidence in the NHS is closely tied to waiting times and access. When people don’t know how long they’ll have to wait or to whom to turn, anxiety grows among the public. Leaders present at the dinner stressed the importance of clear, honest communication with the public – explaining not only what is changing, but why. People want simplicity, not bureaucracy; certainty, not confusion.
Reimagining metrics and accountability
A fundamental rethink of how success is measured was also discussed. Many of today’s key performance indicators are designed for performance monitoring, not for meaningful change. Attendees called for metrics rooted in health economics, place-based outcomes, and patient experience, rather than just ‘activity focused’ hospital throughput or financial balance.
The discussion also explored wider issues of financial governance. Some questioned whether systems should be permitted to run short-term deficits in order to unlock longer-term savings and improved outcomes. Others highlighted the pressing need for greater clarity and transparency in place-based spending—an area where the NHS still falls short. What became clear is that NHS financial structures remain rigid and poorly suited to support innovation or invest in preventative approaches that may not yield immediate performance gains, demand reduction, or visible returns. There is still discomfort within the system when benefits are not directly or immediately felt by the organisation itself.
Stop talking. Start doing
The dinner closed with a sense of urgency. The opportunity presented by the 10-Year Plan is real, but so too are the risks of continued inaction. Siloed thinking, limited risk appetite, and cultural inertia are holding the system back. Leaders agreed that it’s time to stop talking about integration, co-production, and shifting left, and time to start doing them.
This means creating space for genuine community engagement, sharing risk across sectors, and aligning incentives to patient outcomes rather than institutional survival. It means trusting others in the system to deliver value, even when they sit outside the NHS’s traditional structures. Above all, it means holding our collective nerve.