IHOs: Another NHS rebrand? Why ‘integrated care’ is doomed without a financial revolution

For thirty years, the NHS has chased the dream of integrated care through a dizzying series of reforms. The latest buzzword is the ‘Integrated Healthcare Organisation’ (IHO), but it is doomed to fail just like its predecessors, unless we radically reform the financial incentives that pit hospitals against community care. By Lucia De Santis, Consultant at Edge Health.
Ghosts of reforms past: A thirty-year journey of fragmentation
Before the market reforms, District Health Authorities (DHAs) ran the whole show. They planned services and managed the hospitals and community care for their local population. It was an integrated model by design, but it had a fatal flaw. Funding was based on history, not on how many patients were treated, how complex their needs were, or the quality of the care provided. This gave hospitals little reason to innovate or improve, feeding the waiting list crisis of the late 1980s – with median waiting times for inpatient treatment (the only recorded metric at the time) hitting over 22 weeks.
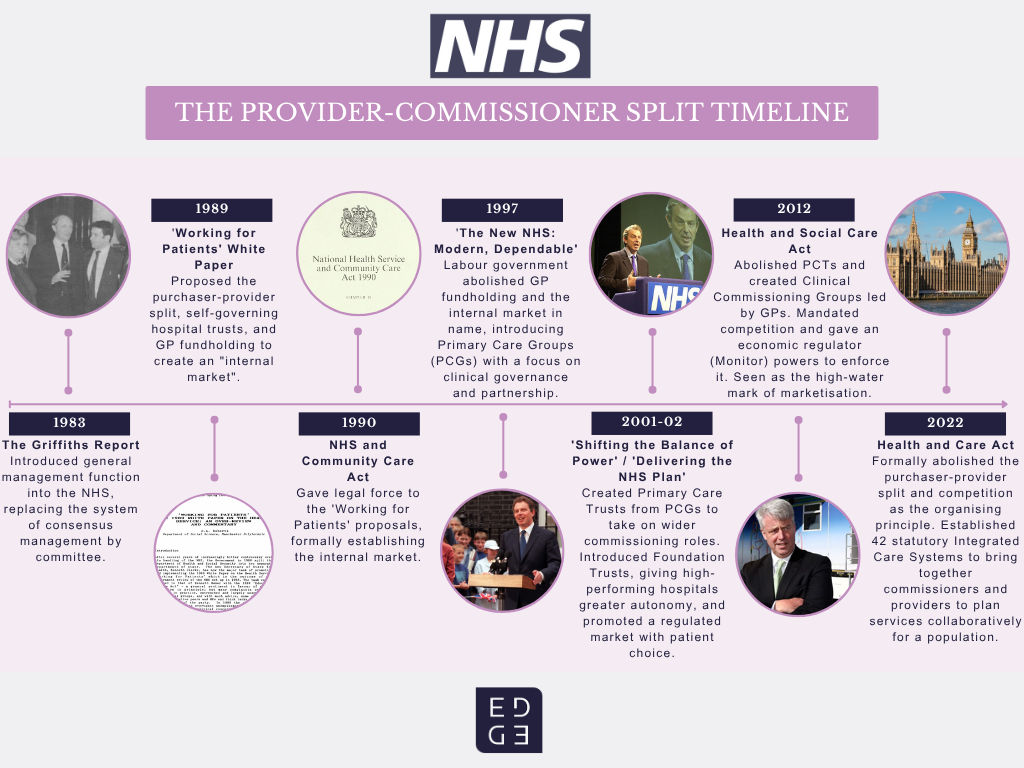
The 1989 Working for Patients white paper blew this model apart, introducing the “purchaser-provider split” that would define the NHS for the next thirty years. The theory was simple: separate the buyers of care (commissioners) from the sellers (providers) and let competition drive everything forward. Money was the carrot – and the stick.
What followed, however, was a dizzying series of reorganisations, as successive governments tweaked the model, moving from GP Fundholding to Primary Care Trusts and finally to Clinical Commissioning Groups (CCGs). This market-based philosophy reached its peak with the 2012 Health and Social Care Act, which put competition at the very heart of the NHS.
The market’s hangover
By the mid-2010s, it was clear the market experiment had struggled to deliver, and left a legacy of fragmentation. One could argue fragmentation has its merits – less bureaucracy, can drive high activity levels (which, until recently, was the key marker of performance). However, fragmentation shows its flaws when it comes to caring for a population with increasingly complex, long-term conditions. This requires seamless coordination between GPs, hospitals, and community services.
Plus, collaboration becomes an even greater struggle when community and secondary care are made to argue over who gets the slice of the pie needed to sustain services. Under Payment by Results, a hospital admission generates income. This wouldn’t be as much of an issue if prices were truly reflective of costs. In reality, costs change with activity (economies of scale) and often prices aren’t set to the actual cost, translating in significant cross-subsidies to sustain “loss-making” services. This creates a perverse, if logical, reality: moving care into the community isn’t just a different way of working; for a hospital trust, it is a direct threat to its bottom line.
The 2022 Health and Care Act officially buried the purchaser-provider split, establishing integrated care systems (ICSs) to bring everyone back to the same table. But while the law changed, the culture (and the money) didn’t. Today’s integrated care boards (ICBs) are left trying to align the priorities of hospitals and community providers in a system still wired for competition and cost management. This has bred a deep-seated scarcity mindset. For decades, providers have been forced to focus on their own financial preservation, diverting energy from transformation to simply keeping the lights on.
And so, we are back to a single organisation – the IHO. However, this model is fundamentally different from ICBs. If the NHS chose to mimic international counterparts, it would mean giving a single provider organisation total control over the budget for a population’s entire care journey. The hope is palpable: under one leadership and budget, integration could finally become a reality.
Making IHOs work: Follow the money
In dismantling the old command-and-control model, the reforms of the past threw the baby out with the bathwater. A single organisation overseeing both hospital and community care is not inherently a bad idea. The mistake was funding them without sufficient accountability*, and the overall lack of focus on performance, need, outcomes (and data!).
If we are serious about making community and hospital services partners instead of economic rivals, giving a single provider organisation responsibility for the whole patient journey feels like the only way forward. But to break the cycle of perverse incentives we must accept that in healthcare, real change follows the money.
The solution is a tough but effective one: change the payment model to make it more financially appealing for organisations to deliver more activity in the community and less in hospitals (where appropriate, of course). This only works, however, under one non-negotiable condition: the IHO must hold the entire budget for both community and acute care for its population and be fully accountable for the level of quality that it needs to deliver. Without this, you unleash the “NHS Hunger Games” – a turf war where providers are locked in a battle for their own survival.
By giving a single IHO control over the whole budget, shifting care from a costly hospital bed to a more efficient community setting** suddenly becomes the most rational financial choice. This requires two bold moves:
- Direct investment: We must supercharge community services to build their capacity. Ideally, this would be an “invest-to-save” model, paying a premium for care delivered out of hospital. A more painful but perhaps necessary alternative would be to pay less for hospital activity that could have been delivered in the community.
- Tied funding: The IHO’s budget must be linked to both population need and performance. Organisations struggling to meet population needs where others in similar contexts (deprivation, demographics) have succeeded would need to be held accountable and undergo greater scrutiny to fix the drivers or be financially liable.
Betting on prevention
One obvious critique of the above is that paying community activity at a “premium” doesn’t actually save any money – at best, if funds are moved away from the acute setting, it would achieve a net neutral scenario. But here’s the key – this shift is not going to suddenly unlock billions of savings overnight. However, it feels like the necessary carrot to drive a behaviour change: invest more in prevention, rather than focus all efforts on treatment. Currently, with a healthcare infrastructure that favours acute treatment from a financial, structural and capital point of view, there’s just not enough incentives to move activity out of hospitals.
Leaders should be making a bet: that a behaviour shift favouring prevention and community care will truly deliver a healthier population. There are very good grounds to believe it true. But we can’t expect an overnight change, that’s not how physiology works. We are unlikely to see true savings for a decade at least – but it’s a worthy investment.

A call for bold leadership
The foundations for IHOs have already been laid by Provider Collaboratives. In places like Cheshire and Merseyside, hospital trusts are already working together at scale – and won an HSJ award in 2023 for working together to eliminate long waits. If these collaboratives were given control over a single, population-based budget and the freedom to reward prevention over cure, we might finally achieve the integration we have been promised for so long.
Of course, that is if we can eventually shift collaboratives towards conglomerates that function more as a unit (operationally, digitally, workforce-y…) rather than a chimera of different interests and operating models.
Navigating this transition will be complex, and leaders will need to be bold, grasp the nettle of financial reform to really build the integrated system that patients deserve, and staff have long been promised, rather than just shuffling chairs on the deck – again.
* In the pre-1990 DHA times, a hospital received its budget as a block grant at the start of the year, and any unspent surplus was often clawed back by the authority, creating an incentive to spend the entire allocation regardless of efficiency. There was no meaningful relationship between the funding a DHA received and the number of patients its hospitals were treating. This offered limited incentives for hospitals to innovate, improve productivity, or take on additional work. Additionally, there was no independent external agent with the power or incentive to challenge its performance. If a hospital was inefficient, its waiting list would grow.
** Research from NHS Confederation found that “On average, systems that invested more in community care saw 15 per cent lower non-elective admission rates and 10 per cent lower ambulance conveyance rates, both statistically significant differences, together with lower average activity for elective admissions and A&E attendances.”
About the author
Lucia De Santis is a Consultant and NHS-trained medical doctor. She is passionate about engaging workforce in healthcare improvements, evidence-based transformation and operational strategy. Her unique insights add depth and human element to data analysis, literature review and visualisation.













