By Leanne Stevens, Abbe Ruston, Laura Hallas Hoyes
It is estimated that more than a million people in the UK have lower limb ulceration. With their 160 years’ experience in developing wound care solutions, L&R hypothesised that a self-care delivery model could both improve outcomes and ease the burden on the healthcare system.
L&R has more than 160 years of experience in developing outstanding wound care and compression therapy solutions. They are passionate about transforming outcomes in leg ulcer service provision to support the NHS, the nursing workforce, and patients. Working in partnership with organisations, L&R supports them to drive the self-care agenda, which frees up resources, reduces appointment times and clinic costs, and releases nursing time to care.
Lower limb ulceration is a common cause of suffering in patients and its management poses a significant burden on the NHS, with venous leg ulcers (VLUs) being the most common hard-to-heal wound in the UK. It is estimated that more than one million people in the UK have lower limb ulceration, of which 560,000 are categorised as VLUs. Much of burden of VLUs currently sits within the community and primary nursing workforce, with up to 50 per cent of community nursing workload being taken up by chronic wound management.
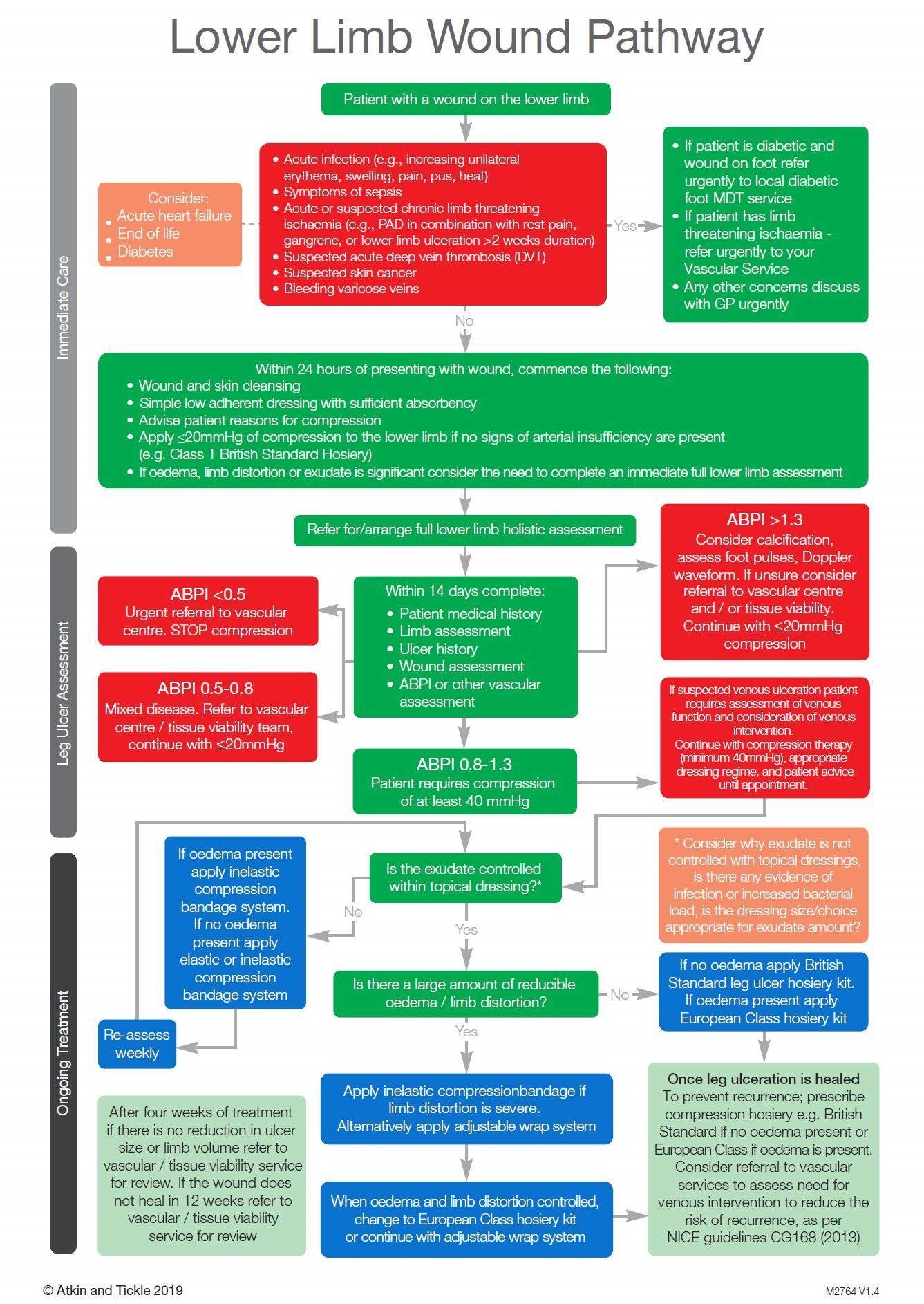
In South West Yorkshire Partnership Trust (SWYPT), it was hypothesised that a self-care delivery model, in partnership with the Leg Ulcer Pathway could reduce wound care burden on the health service and improve patient empowerment, with little or no reduction in healing outcomes.1 Therefore, L&R, in partnership with SWYPT, created a project called the “Big Squeeze”, with the aim of delivering transformative outcomes for venous leg ulcer care, achieving a big squeeze on its financial burden and unwarranted variation in treatment and outcomes.
This was implemented through L&R’s three-step approach:
Implementation of a best practice leg ulcer pathway1 – ensuring the right treatment for the right patient at the right time in line with the National Wound Care Strategy Programme recommendations.
Service efficiencies – driving clinical and health economic outcomes through adoption of the self-care delivery model.
An education and coaching programme – for patients and clinical workforce to embed sustainable practice.
Click to enlarge
Evidence of success
95 patients were enrolled into the service evaluation, and:
VLUs of 84 patients had healed by week 24 on the pathway.
VLUs in a further 10 had healed by week 42.
One remaining patient reached 42 weeks without healing.
Comparing the results of implementing the Best Practice Leg Ulcer Pathway in isolation and the Best Practice Leg Ulcer Pathway and the Self Care Delivery Model combined:
Nursing hours per patient reduced from 24.5 to 1.3, releasing up to 95 per cent in nursing hours.
Total cost per patient reduced from £2,168 to £361, saving up to 83 per cent in total cost of care per patient.
Product cost per patient reduced from £629 to £177, saving up to 72 per cent in product costs per patient.
In addition to healing and financial outcomes, improvements in staff motivation and wellbeing were recorded through survey feedback, as well as 1,471kg saving in C02 per 100 patients through a reduction in miles driven by the community workforce.
Report finds total number of retired benefits recipients likely to rise by 60 per cent in next decade, with costs expected to rise to £10.5bn.
A significant increase in the number of people spending a decade or more of their retirement on disability benefits is expected unless urgent preventative action is taken, according to new research from consultancy firm LCP.
Although much of the public discussion around ‘economic inactivity’ focuses on those of working age in receipt of benefits for those unfit to work, these benefits stop at pension age, when individuals switch to a state retirement pension. By contrast, disability benefits such as Personal Independence Payments (PIP) continue to be paid throughout retirement for those already eligible when they retire. The new analysis suggests that unless action is taken to improve the health of these individuals, the cost of funding these benefits will rise significantly in the coming years.
The research finds that just under 100,000 people aged 66 (the state retirement age) are currently in receipt of PIP or its predecessor, Disability Living Allowance (DLA), and are expected to draw these benefits for another 11 years, on average. It estimates that of those individuals, half will continue claiming PIP until they die. The total payment per person would be around £70,000, but this could rise for individuals on low incomes and those claiming means-tested benefits.
Without mitigation, the total number of pensioners on PIP/DLA is likely to rise by around 60 per cent in the next decade, from approximately 1 million now to 1.6 million in 2023, LCP’s research suggests. The total cost of funding these benefits would rise from around £6bn to £10.5bn.The total current cost of PIP in 2023/24 is £21.8 billion, and the benefit is paid to 3.2m people.
The number of adults in receipt of PIP (plus DLA) has risen by around 1 million in the last decade and is forecast by DWP to rise by another million in the next three years. For younger PIP recipients, the fastest growing reported health condition is mental health problems, whereas, for older claimants, it is more likely to be musculoskeletal complaints. The fastest growing group of recipients is those who have been in receipt for five years or more, suggesting a risk of a large and growing ‘core’ of recipients with a dwindling prospect of flowing off benefit at all.
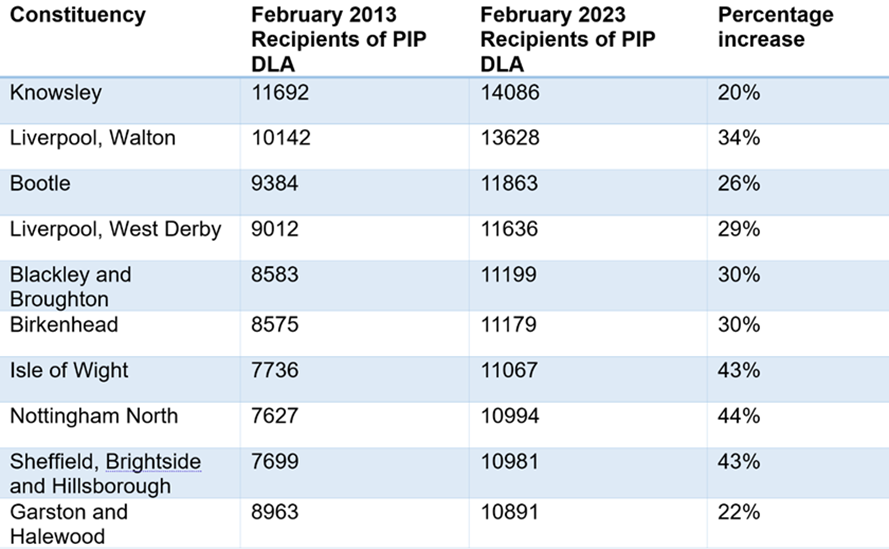
Looking at all PIP/DLA recipients aged 16 or over, receipt of benefits is heavily concentrated in more deprived areas. The table (below) shows the 10 parliamentary constituencies with the highest absolute numbers of PIP/DLA recipients as of 2023, and how the number has changed in the last decade. Five of the top six are in the Merseyside area, and all have seen a growth in numbers of between 20-30 per cent in the last decade.
If targeted action is not taken, many of the working age claimants in these areas will reach pension age on disability benefits and then be more likely to die in receipt than cease claiming.
Table: Westminster constituencies with largest numbers of 16+ recipients of PIP / DLA in 2023 (England and Wales only). Source: DWP ‘Stat Xplore’ database. Click to enlarge.
The higher levels of benefit receipt in more deprived areas suggest the potential for targeted health interventions, which could reduce the number of people who need to claim in the first place and/or reduce the length of claim for those who do receive benefits. However, the authors argue that past government interventions have proven insufficiently focused on those most in need.
The research cites as an example the DWP’s recent expansion of the “Individual Placement and Support in Primary Care Programme” (IPSPC), which was designed to support individuals in receipt of disability benefits. However, the list of local authorities chosen to date excludes those where disability benefit receipt is at its highest.
Another example is NHS England’s ‘Elective Recovery Programme’, which aims to increase capacity to tackle the waiting list backlog that significantly worsened during the Covid-19 pandemic. This programme has not specifically prioritised areas of greatest unmet health need, according to the researchers.
The paper argues that with each person who reaches pension age on PIP likely to receive another £70,000 in benefit on average, there is great potential for cost-effective interventions which would benefit the individuals concerned as well as the taxpayer. For example:
Clinically recommended Diabetes meters for those with Type-2 Diabetes cost just £5.50 each; roughly 13,000 such meters could be funded from the savings of just one person fewer needing PIP through retirement.
Where people have mental health problems alongside physical problems, low intensity psychological treatments have been demonstrated to be a cost-effective method of treatment. The cost of such ‘collaborative care’ is around £2,140 per person, a fraction of the potential cost saving of £70,000 through avoided benefit payments.
Commenting on the results, co-author and Head of Health Analytics at LCP, Dr Jonathan Pearson-Stuttard, said: “The prospect of large numbers of people going into retirement facing long-term disability benefit receipt is not in the interests of the individuals concerned or the taxpayer. If just one less person needs to claim Personal Independence Payment through retirement the saving is likely to be around £70,000 and that money could be much better spent keeping people well and supporting those who have disabilities. More targeted interventions, particularly focused on areas of greatest deprivation and highest health needs, could pay off many times over in terms of benefit savings and gains to the wider economy.”
Why healthtech providers to the NHS have a responsibility to design interoperable solutions
By Dr Anas Nader
Boosting access to innovative technology has never been more important for the NHS. But providers have a duty to ensure interoperability is at the core of all solutions, writes Dr Anas Nader.
With the NHS facing increasing challenges, from extensive waiting lists to rising staff burn-out, boosting access to innovative technology across the industry is becoming a growing priority. The Health Secretary has promised to ringfence funding for health tech, highlighting it as a key investment for the future of the health service; and there is no shortage of emerging tech offering to step to the fore and build new solutions.
Many are already shaping up to deliver on this promise – from remote patient monitoring to increased surgical accuracy. But there is one thing that must not be overlooked: if these solutions are to have a long-term tangible impact, and support more joined-up care delivery across new integrated care systems (ICSs), they must be designed with interoperability in mind.
An interoperable solution is one that can connect with other systems, allowing for information to be easily and safely shared without the need for manual intervention. With hundreds of digital systems in use across the NHS – including databases such as the Electronic Staff Record – new tech must be able to ‘speak to’ these and share information directly if it is to have a viable long-term benefit. This is especially vital for facilitating cross-service collaboration within ICSs, enabling systems at different organisations to effectively and securely send information to each other.
For this reason, NHS England has identified interoperability as a key area of focus, to help boost the capabilities of ICSs, which were set up to drive the shift towards more joined-up care. This is a goal echoed by other recent reports, including the Hewitt Review, which highlights the importance of joined-up care and the effective interchange of information across organisational boundaries.
While new healthtech innovations are often built with the best of intentions, tech that cannot be successfully used in conjunction with other systems can inhibit this much-needed collaboration. Whether that’s by creating silos which slow down communication or increasing the admin burden on clinicians by requiring data to be manually re-entered; without interoperability, new technology can become difficult to use, and ultimately risks being abandoned by the clinicians it was built to support.
Indeed, a lack of interoperability between systems has been flagged as an ongoing problem in the NHS, with 76 per cent of doctors viewing this as a ‘significant barrier’ to digital transformation. According to the BMA, 13.5 million working hours are lost in England each year as a result of fragmented tech and IT systems.
To create a successful product that can make real change in the NHS, and facilitate genuine ICS-wide collaboration, healthtech companies must take into account the complex ecosystem of healthcare IT systems within the NHS. Providers have a responsibility to build in a way that ensures our solutions deliver genuine interoperability as standard.
How healthtech providers can deliver on interoperability
The biggest mistake that health innovators building tech for the NHS can make when approaching interoperability is viewing their product and the NHS as completely separate entities. Rather than being built for and with the NHS, solutions are often built in isolation, and then have to be retrofitted to meet the needs of each ICS. This is a surefire way to create a tech solution that is inherently incompatible with other NHS systems. To avoid this, companies must build in a way that prioritises interoperability from day one, with a close appreciation for the other systems tech must work alongside.
In the same vein, innovators must ensure their solution can be adapted to the many different healthcare contexts in which it could be used across each ICS. It may need to communicate with systems in primary care, hospitals, outpatient settings, or community and mental health care services. Ensuring full interoperability will allow for greater flexibility and mean it can be successfully adopted in different settings across ICSs, facilitating effective cross-service collaboration as a result.
Interoperability is not a ‘one and done’ exercise. Within systems as complex as the NHS, tech solutions must be flexible and able to continually evolve to meet the changing needs of the services using them. Healthtech companies should provide ongoing technical support and remain on-hand post-implementation to ensure that the solution continues to be a success. Parachuting in tech without this continued support may simply place a shelf life on the solution, especially if it is unable to integrate with future systems that are brought in across the ICS.
If technology is to fulfil the needs of the NHS’s staff and patients, interoperability must be prioritised at every step. This is vital for ensuring that the solution helps, rather than hinders, the healthcare service and offers a long-term solution which enables effective collaboration within the ICSs using it.
A failure to design interoperable software will result not only in an increased burden for NHS staff, but a lack of adoption and success. It’s a two-way street: working in partnership with the NHS to ensure systems are able to embrace new technologies is key. But innovators must actively take up the charge to prioritise interoperability and build solutions equipped to effectively support more ICS-wide, joined-up care.
Dr Anas Nader is the Co-founder and CEO of Patchwork Health: a digital solution that connects NHS organisations to a growing number of healthcare workers, reducing the reliance on locum agencies and improving the experience of flexible working in the NHS.
Winter is coming: how Doccla’s virtual ward pathways support Urgent and Emergency Care
By Tara Donnelly
Tara Donnelly, Founder of Digital Care Limited, explains how Doccla is supporting NHS Urgent and Emergency Care through an innovative suite of virtual ward and remote patient monitoring technologies.
Emergency Departments (EDs) across the NHS in England have experienced another record-breaking year, both in terms of increased volumes of patients attending – more than 24 million emergency attendances – and decreases in performance against waiting time standards. Pressures on EDs are no longer seasonal but exist all year round, leading to adverse patient experiences. It is imperative that all those involved reimagine how Urgent and Emergency Care (UEC) services are delivered to support NHS colleagues who are bracing for a challenging winter ahead.
There is increased recognition that digital solutions could help to alleviate some of this burden. NHS England’s latest guidance to deliver the UEC Recovery Plan spotlights the expansion of virtual wards as a high impact intervention this winter. Doccla, a leading provider of virtual wards and remote patient monitoring, is working closely with its NHS partners to provide alternatives to admission and to relieve bed congestion by supporting early discharge. The team works with more than a third of integrated care boards, providing:
A customised suite of technology to help clinicians and carers monitor patients at home.
Clinical dashboards that enhance caseload management through holistic views of patient cohorts and visualisations of patient data trends over time.
Integration with electronic patient records to enable flow of coded data from the Doccla dashboard to the patient’s medical record during their stay on the virtual ward.
Access to multi-disciplinary clinicians with specialist training in remote monitoring.
An end-to-end logistics service that task-shifts administrative and non-clinical activity from busy clinicians.
Access to a patient support team, which uses a variety of accessibility tools to ensure patients from all demographics are aptly supported on virtual wards, from onboarding through to discharge.
Doccla’s technology has been pivotal in enhancing various admission avoidance pathways within UEC settings.
Remote monitoring available to community urgent response teams
Doccla’s technology is integrated within Hertfordshire Community NHS Trust’s (HCT) virtual ward service. Under the guidance of HCT’s Medical Director, Dr. Elizabeth Kendrick, the service has enabled the rapid assessment, diagnosis, early treatment and discharge of over 4,000 patients – recently winning a Parliamentary Award for its work.
Hertforshire Community Trust’s Hospital at Home service, using Doccla technology, has recently won a Parliamentary Award for its work.
Most recently, the technology has been deployed to HCT’s urgent care and response teams tackling ambulance wait times. Rather alarmingly, one in 10 ambulances spend more than an hour waiting outside hospitals. Joining forces with the East of England Ambulance Service, HCT equipped its community urgent response service with Doccla remote monitoring boxes so they could have an additional tool to support people to stay at home. Early evaluation of the pilot showed promising results, including:
Reduced ambulance conveyance rate to 33 per cent (from an anticipated 100per cent conveyance rate).
Reduced ambulance attendances by 18 per cent at East and North Herts NHS Trust.
Increased time available for crew to respond to acute emergency calls.
Reduced handover delays outside hospital.
Tackling surges in respiratory admissions this winter
Seasonal variations in respiratory admissions are a major contributor to pressures within emergency care settings over winter. There are 80 per cent more lung disease admissions in the winter months of December, January and February than there are in the warmer spring months of March, April and May.
Virtual wards provide an alternative mechanism for services to manage patient flow and to cope with the surge in respiratory admissions. The Doccla-supported ARI pathway at Northampton General Hospital (NGH) has demonstrated considerable efficiencies for the delivery of care. By supporting early discharge, NGH’s virtual ward service achieved:
11 per cent reduction in length of stay.
30 per cent reduction in bed days.
Likewise, tech-enabled remote monitoring enabled earlier detection of, and interventions for, deteriorating patients, resulting in a 15 per cent reduction in readmission.
While additional UEC funding has been injected into integrated care systems, allocation of monies is challenging when there are competing needs across care settings. It is paramount that the additional funding is maximised. NGH’s virtual ward service demonstrates a £13,000 per month saving (associated with the reduction in bed days) and more broadly, has enabled workforce capacity savings. Analysis in 2021 showed on non-tech enabled wards, there is 1 nurse per 8.3 patients on average. Doccla’s tech efficiency gains have expanded this to 1 nurse per 10 patients.
Augmenting SDEC services
Bristol, North Somerset and South Gloucestershire (BNSSG) is another example of how effective partnership between clinical and operational teams, in conjunction with Doccla’s innovative technology, can reduce admission rates. Between February and May this year alone, BNSSG’s NHS@Home service:
Provided an alternative to admission or supported earlier discharge 487 times.
Enabled local people to be cared for at home for an additional 4442 days
Supported cost savings of £1,479,186.
Avoided readmission for 87 per cent of patients.
In collaboration with Doccla’s remote monitoring technology, BNSSG NHS@Home teams are pioneering the use of remote monitoring for same day emergency care (SDEC) patients to avoid inpatient stays within North Bristol Trust – with the SDEC model contributing approximately 20 per cent of NBT’s weekly referrals to the NHS@Home service.
An example of a presenting condition being cared for in this way is the bacterial infection Cellulitis, which results in more than 100,000 hospital admissions per year in England alone. The new pathway has the patient set up for remote monitoring while in the hospital; they are given a Doccla box to take home and asked to send in their readings over the next few days, to indicate to the clinical teams whether or not the infection is under control. Given that 1.6 per cent of all NHS hospital admissions are due to Cellulitis, enabling speedy discharge or reduction of inpatient stays for patients with the condition has the potential to shift the dial on bed pressures this winter.
Conclusion
It feels important both for patients and the sustainability of the NHS that we do everything in our power to rapidly scale innovative solutions that are demonstrating impact in tackling pressures in Urgent and Emergency Care pressures.
As a trusted partner to health systems and providers, Doccla’s technology is being flexed in agile and impactful ways to support urgent care pathways this winter.
If this has sparked ideas that you are keen to action locally, please reach out to the Doccla team here. Doccla will be attending Public Policy Projects’ ICS Delivery Forum on 4th October to continue the conversation.
People with severe eczema face a hidden cost of living crisis
By Rippon Ubhi, Sanofi Specialty Care General Manager
New report from Sanofi shines a light on the hidden financial burden faced by sufferers of severe atopic eczema.
Nearly everybody has felt the pressures of the cost-of-living crisis. Prices rising, bills soaring, and having to do more with less. This is a real concern for so many, but it’s even worse for people living with uncontrolled atopic eczema, who have to contend with additional costs, both direct and indirect, which are causing a significant strain on both individuals and the healthcare system.
Atopic eczema – known medically as atopic dermatitis (AD) – is the most common form of eczema in the UK, affecting 5-10 per cent of all adults, and causing the skin to become itchy; during a flare-up it can become red, cracked and sore. From the financial costs of medications to an increased risk of developing depression, the costs of uncontrolled eczema to many people living with the condition are wide-ranging and detrimental to their quality of life, particularly for people from lower socioeconomic backgrounds.
Eczema can often be overlooked as a healthcare issue by the general public, and Sanofi recognises the significance of highlighting the genuine effects on the individual that it can cause. Sanofi’s aim is to increase awareness and shine a light on the true cost of the condition. So, we commissioned leading cross-party think tank Demos to produce a report which analyses the impact that uncontrolled atopic eczema has on patients, the NHS and wider society.
The Costs of Atopic Dermatitisreport, published in April 2023, draws on an evidence review of UK and international literature, interviews with clinicians in England and the experiences of people living with eczema to examine the costs, the current state of patient care and how patient care can be improved.
The financial burden of eczema
The report provides insights into the costs borne by people living with uncontrolled eczema. This financial burden is far more significant than many might expect. One clinician Demos interviewed said that sometimes patients with lower socioeconomic status have to make a choice between paying for medication or buying food. This cost to society goes beyond just the healthcare system, hitting the economy as a whole. In the UK, the indirect costs of work impairment to the economy for adult patients with moderate-to-severe atopic eczema is estimated to be between £6,741-£14,166 per patient, per year.
But why does it cost so much? Firstly, people living with severe eczema have to spend money on both medical and non-medical items such as medicines, emollients and moisturizers. The impact the condition has on their ability to work also adds to the personal financial cost. Patients with severe, uncontrolled atopic eczema often need to take additional sick days and they may even lose work because of their condition. Then there are the intangible costs: people living with eczema may have to deal with sleep impairment and other mental health issues exacerbated by the irritation and appearance of their skin.
There is an impact on the NHS too. The direct cost of mild-to-moderate eczema to the health service was estimated as being at least £257m in 2020, though there have been no comprehensive studies encompassing the costs of severe atopic eczema. It is estimated that around 15-20 per cent of GPs’ workload is dermatology, with a large quantity of that work being eczema.
Reforming dermatology pathways
The Costs of Atopic Dermatitisreport has shone a light on the problem. We now need to focus on how we can alleviate this financial burden. That means investment in improvements to the standard of care for people living with atopic eczema, to drive positive outcomes for patients and reduce long-term costs to the health service and the economy.
If integrated care systems develop dermatology strategies and ensure that psychological support is commissioned as part of the dermatology pathway, these costs can be significantly reduced, by lessening the mental burden of eczema. We as a country need to do more to ensure that healthcare professionals know about the full range of support available to patients. It is vital that patients feel supported by their doctors to access mental health care where appropriate, and that GPs have the training and resources needed to provide the best care possible to their patients with eczema.
Through commissioning this report, Sanofi hopes it has played some small part in bringing the issue of atopic eczema and its cost to us all into relief. The next steps, however, need to be taken by decision makers as they decide whether they want to act to rescue the costs of eczema to patients and our healthcare system.
Report finds doctors and nurses ready to embrace generative AI
By Integrated Care Journal
Elsevier Health’s landmark Clinician of the Future 2023 report highlights new opportunities technology will play in providing relief for healthcare workers and geographical differences in opinion
Global information and data analytics leader, Elsevier Health, has today released its Clinician of the Future 2023 report, offering a snapshot view on what doctors and nurses think about the changes and current challenges in healthcare, including the rapid rise of generative AI products and platforms.
The report finds that nearly half of all doctors and nurses surveyed are eager to make use of these new technologies to support their clinical decision-making. While only 11 per cent of today’s clinical decisions are assisted by generative AI tools, 48 per cent of respondents said that doctors using these tools to help make clinical decisions will be ‘desirable’ within two-three years’ time.
The current study comes one year after the launch of the inaugural Clinician of the Future report, which aimed to provide a voice for clinicians and a mandate for change to help ‘future-proof’ the global health industry. This new report canvassed the views and opinions of 2,607 doctors and nurses worldwide, building upon the understanding of healthcare workforce challenges highlighted in the original survey, but now putting an additional lens on the future of generative AI technologies across global healthcare.
Participants across both Clinician of the Future reports spotlight concerns around overwhelming resource issues for healthcare systems worldwide, even as they face substantial treatment backlogs. Clinician shortages remain the top concern in North America and Europe, with 54 per cent of clinicians surveyed for the 2023 report identifying nurse shortages as a pressing health priority.
“73 per cent of doctors surveyed believe they themselves will need to be experts in the use of digital health technologies…within the next two-three years.”
45 per cent similarly reported the need to tackle doctor shortages, reinforcing the urgent need for innovative solutions, such as generative AI, to address clinician shortages, as well as identifying opportunities for efficiencies and training to both enhance clinical readiness and provide much needed clinician support.
Additionally, doctors surveyed believe that they will themselves need to be experts in the use of digital health technologies, with 73 per cent of clinicians agreeing that these skills will be ‘desirable’ within the next two-three years. Accordingly, 55 per cent expressed as ‘desirable’ the transition towards ‘telehealth’, agreeing that remote routine checkups should form the majority of patient-clinician interactions within the next 2-3 years.
While more than half (51 per cent) of clinicians welcomed the prospect of medical students using generative AI-powered tools as part of their medical education in the next 2-3 years, clinicians from the UK and the US were found to be more reserved about generative AI technologies supporting medical students; only 33 per cent in the UK and 40 per cent in the US found this ‘desirable’.
Jan Herzhoff, President of Elsevier Health said: “As healthcare systems continue to face significant challenges, we must raise the voices of doctors and nurses worldwide to understand how we can best support them and the patients they care for. In this pursuit, advanced technology combined with trusted medical content emerges as a powerful ally, and generative AI, particularly, shows immense promise in helping clinicians.”
Mr. Herzhoff added: “By equipping clinicians with advanced tools and training to support their clinical decision-making, doctors and nurses will be empowered to allocate more time to the human aspect of patient care.”
As global healthcare systems progress towards a more digital-first approach, the findings in the Clinician of the Future 2023 report demonstrate that the workforce not only recognises the potential new technologies like generative AI can provide to innovate global healthcare, but also their beneficial impacts on patient care.
Josh Schoeller, President, Global Clinical Solutions at Elsevier and CEO, Healthcare at LexisNexis Risk Solutions said, “Elsevier is renowned for powerful point-of-care solutions that support clinicians throughout their workday. We have been at the forefront of developing clinical solutions tools, prioritising the responsible use of AI, while anticipating and staying ahead of the latest technology trends. We are deeply committed to listening to the needs of clinicians so we can continuously enhance our products to create efficiencies, enabling clinicians to prioritise delivering life-saving care.
For the full ‘Clinician of the Future 2023’ report, which includes robust data on global attitudes on the future of healthcare, important insights on training and development and more, click here.
Building a culture of transparency and accountability will be essential steps to encourage and protect whistleblowers in the speak-up system.
The NHS has been grappling with concerns surrounding its whistleblowing systems and cultural health. This has been highlighted repeatedly in the press over the last week with coverage of the Lucy Letby trial, within which there were shown to be multiple failures in internal reporting processes.
This demonstrates the need for an independent reporting line for employees across the organisation. NHS employees must have the opportunity to speak with an entirely impartial party who can process their concern and pass on the information to the appropriate team for further investigation.
Whistleblowers within the NHS have often faced challenges, making them hesitant to report wrongdoing due to fears of retaliation and detrimental treatment. Despite these obstacles, 2023-23 saw a significant increase in NHS whistleblowers coming forward compared to the previous year, highlighting the urgent need for reform in the whistleblowing process.
In fact, a record 25,000 plus NHS whistleblowers came forward last year. Of these cases, as has been reported by Freedom to Speak Up Guardians office, the most common reports were of inappropriate behaviours and attitudes (30 per cent), followed by worker safety and wellbeing (27 per cent) and bullying and harassment (22 per cent).
Reports indicate that NHS employees are lacking confidence in the current speak -up system, with many feeling labelled as troublemakers when they raise concerns. This detrimental culture not only deters individuals from speaking up but also hinders the NHS’s ability to identify and address wrongdoing, potentially endangering both patients and employees. And that’s before the damage to the NHS’s reputation is considered.
Improving the speak-up system
For optimal trust and confidence in a speak-up system, employees must feel that their concerns will be taken seriously and investigated appropriately.
Unfortunately, this most recent case is the most extreme example of that not happening, with Dr Stephen Brearey stating that if hospital executives had acted on concerns about nurse Lucy Letby earlier, lives may have been saved.
To address these pressing issues, steps need to be taken to: improve employee confidence; identify and combat wrongdoing; and protect those who come forward to report concerns.
One crucial measure is to review and audit the NHS’s whistleblowing policy, processes, and operations to understand the reasons for the breakdown of trust. Identifying and holding accountable those responsible for retaliating against whistleblowers is essential to foster a culture of transparency and accountability.
Providing whistleblowing training to both employees and managers is another critical step to improve the speak-up culture. When employees are aware of how to raise concerns, and the legal protections they have under the Public Interest Disclosure Act (PIDA), they are more likely to come forward without fear of retribution. Additionally, providing training to managers on how to receive and handle disclosures appropriately can help deter misconduct.
The current Freedom to Speak Up (FTSU) Guardian scheme, while a positive step towards improving whistleblowing culture, appears to lack confidence among NHS employees, with many remaining hesitant to report serious concerns through an internal system due to doubts about confidentiality and impartiality. One worker told the FTSU Guardians that “the Guardian was excellent, but nothing has been resolved”. The Guardians themselves have said that managers need to be trained about their obligations once they receive a report.
Taking affirmative action to instil trust
To build trust, the NHS can consider offering an alternative means of disclosure, such as a dedicated, outsourced whistleblowing hotline provider, ensuring true anonymity and independence in the reporting process. Safecall already works alongside several NHS Trusts helping make their processes more robust and transparent. Employees are much more confident speaking to, and reporting through, a third party.
It is vital that the investigation procedure is handled in a fair and balanced fashion, and not conducted in a way that undermines the whistleblowers’ concerns. To instil confidence in the reporting process, investigations should be conducted in an independent and confidential manner. Outsourcing the investigation process or ensuring that internal investigators undergo proper training and possess the necessary experience can help safeguard employees’ wellbeing and protect the NHS’s reputation.
It is paramount for the NHS to take affirmative action in protecting whistleblowers and fostering a culture of transparency and accountability. No healthcare professional should face detrimental treatment for raising concerns that may impact patient safety. To achieve this, the NHS must review its systems, provide comprehensive training, and offer reliable and independent reporting avenues.
The NHS must strive to offer confidentiality, impartiality, and independence when receiving and investigating concerns. These efforts should be continuous and consistent to create effective and sustainable change within the organisation.
In conclusion, addressing whistleblowing concerns in the NHS is crucial for promoting a culture of transparency and accountability. By taking proactive steps, such as reviewing policies, providing comprehensive training, and ensuring independent investigations, the NHS can create an environment where employees feel confident and protected when speaking up against wrongdoing.
Fostering a culture that values whistleblowers and their contributions will not only strengthen the NHS internally but also enhance its reputation and commitment to patient care.
Chancelle Blakey, Business Development Manager, Safecall
NHS Workforce Plan will need a change in mindset from clinicians, patients and systems
By Amanda Grantham
Enacting reforms through a clinically-led, multi-disciplinary lens will be critical to achieving the ambitions of the NHS Long Term Workforce Plan.
The NHS Long Term Workforce Plan centres on the need to train, reform and retain its employees to meet future demand, leading to an increase of up to 360,000 new staff across integrated care systems (ICSs). Increasing the number of formal training places available through more diverse points of entry and improving retention through rewarding career and development are at the heart of what needs to be done to deliver this plan.
The introduction of new roles, reforming the way care is delivered and by whom, will be critical to meeting anticipated demand in 2036/37. But these roles will need to be designed, clinically-led, and committed to driving productivity to create the capacity needed.
Determining which roles will be needed to meet demand
It is important to recognise that more staff will not increase capacity unless clinical pathways can be redesigned to be more efficient and effective. During COVID-19, there was about a 10 per cent increase in headcount within NHS acute trusts. However, at the beginning of 2023/24, providers were at 97 per cent of pre-pandemic productivity levels. Delivery of the NHS Workforce Plan means broadening the skill mix of multidisciplinary teams, creating new and diverse roles across systems. In designing the new workforce, the roles need to create new capacity to meet demand, either through new services to meet future need or by increasing provision in existing services.
Creating a new role requires the redesign of the way that multidisciplinary teams work together. The starting point for this workforce design should be the optimal clinical pathways, rather than what is being done today. That means setting out the clinical red lines (what can only be done by a registered healthcare professional), looking at the skills and roles needed, and the most efficient use of capacity.
The design of the COVID-19 vaccination workforce demonstrated how new roles could be created to meet increased demand. The drive to create this workforce led over 145,000 people to join the NHS working as unregistered vaccinators who came from diverse backgrounds, including retired medical staff, airline workers, volunteers and students.
Systems will also need to be more focused on the competency of the workforce, training employees in the skills needed to deliver their role safely and efficiently. The aim from the offset should be designing broad and rewarding recruitment, training and career pathways that will attract and retain the right talent. This could include consideration of how these roles can be steppingstones into future training or careers, as well as how apprenticeships could open doors for eligible people to take on these new roles.
To meet growing demand in the national breast screening programme, two unregistered roles have been created in collaboration with the College of Radiographers, along with redefined roles and clinical career frameworks. Approximately 30 percent of the breast screening workforce is now in these new roles. – mammography associates and assistant practitioners – with defined scopes of practice and accreditation to undertake mammography.
Clinical leadership is required
Creating new roles in healthcare is about shifting care, or elements of decision making, to another trained and competent healthcare professional. This requires a change in approach from the provision of clinically delivered care to a position where healthcare is clinically-led but can be provided by a diverse multidisciplinary team. Clinicians should be at the centre of the redesign of the workforce, but their input will need to be coupled with that from those with the skills and expertise in increasing capacity.
The NHS has had mixed success in integrating new roles into healthcare teams. The COVID-19 vaccination programme was a nationally designed workforce model which used simulation to provide an evidence base and was clinically-led.
Another approach, the Additional Roles Reimbursement Scheme (ARRS), was established in 2019 and produced more variable results. The scheme provided an automatic funding stream to Primary Care Networks to recruit 26,000 alternative roles to expand service provision and reduce patient waits.
This was part of the government commitment to improve access to general practice and included roles such as clinical pharmacists and technicians. Not all practices have seen the anticipated benefits of these roles, with the Kings Fund highlighting that the roles were not being implemented or integrated into primary care teams effectively.
It will also be important to manage the expectations of patients, in particular that they will always see a medical professional. The government and NHS leaders need to consider how to secure public acceptance of self-management for those with long term conditions, more care being provided in the home and community rather than hospital, and from trained staff who are not medically qualified. However, there will need to be a visible improvement in access to healthcare services if the public are to support these changes.
The NHS is aiming to have 10,000 virtual ward beds in place to support growing demand this winter. A clinically-led redesign of the workforce means that care will continue to be overseen by a medical team, but the delivery of healthcare will predominantly be through a multidisciplinary team of healthcare support workers and allied healthcare professionals.
New capacity will be needed to meet training demands
The Workforce Plan contains a commitment to grow the number of training places across all professions. Capacity to provide this training will need to be created from existing workforces and services. This creates a risk that waiting times may increase.
The plan commits to growing the number of medical school training places from 10,000 in 2028/29 to 15,000 by 2031/32. Each of these training place will require support from existing clinicians. The British Medical Association (BMA) recommends additional non-patient facing time to support trainees, of only an hour a week, per trainee, for each consultant.
To meet this standard will require more than 125 full time consultants/GPs to be released each year from NHS services. By 2036/37 this will see more than 625 full time consultants/GPs supporting additional trainees, rather than delivering care. That makes it critical that productivity and efficiency are at the heart of service redesign to minimise the impact on waiting times.
This underlines that the plan’s ambitions on training and retaining staff will not be achieved without fundamental reform. That will require a careful analysis of the right size and shape of the workforce that will be needed to meet future demand for local populations. Now more than ever, diverse, multidisciplinary, efficient, and clinically-led approaches will be the key principles that systems should be adopting when driving the reform of their workforce.
Written by Amanda Grantham, healthcare expert and Partner at PA Consulting.
Protecting the dignity of vulnerable people through technology
By Gavin Bashar
Gavin Bashar, Managing Director at Tunstall Healthcare, discusses why it’s important to protect the dignity of vulnerable people and how technology can be used to achieve this while improving health and care outcomes.
As the health and care needs of our population change, it’s important to uphold the dignity and rights of those who use health, housing and social care services. There are a number of strategies and innovations that providers can implement to help them deliver high quality services that support the dignity of vulnerable people.
Protecting the dignity of vulnerable people
As the health and care needs of our population change and the number of older people increases, it is important that service providers understand why and how care provision can play a crucial role in protecting the dignity of vulnerable people.
Dignity can be defined as the state of being worthy of honour and respect. When it comes to health, housing and social care services, this particularly focuses on being able to provide care that is tailored to meet the needs of each individual, their circumstances and wishes.
Robust and integrated systems can be well placed to deliver improved outcomes for citizens, reducing their need for emergency and more extensive care, such as hospital admission. The longer that people are able to remain independent without the need for acute services, the more their dignity and quality of life will be protected.
The role of technology
One of the prime objectives for technology-based solutions is to put people at the heart of their own health and care needs, protect their independence and dignity, and achieve citizen-focused outcomes. With the right digital frameworks in place, services can become focused on engaging each individual with their own health and care support.
When technology is embedded seamlessly into care and support services, it can be transformative, helping people to live happy, fulfilled lives in their homes and communities. Digital tools can also be used to ensure timely and appropriate responses to emergency events, encourage greater engagement from citizens, and provide more person-centred care.
Developments in the provision, scale and quality of digital technology can support improvements in how care providers are able to collaborate and provide person centred care. The UK’s transition to a digital communications network brings a once-in-a-generation opportunity to modernise, improve and shift the sector and its thinking from a reactive, to a proactive delivery model. This in turn can improve health outcomes for citizens, deliver efficiencies, and enable people to live independently for as long as possible.
Investment in digital solutions will support health and social care providers in reconfiguring services to make them more agile and integrated, leading to better outcomes. Utilising data and technology to create a connected approach can also provide actionable insights to deliver more informed, and more effective care.
Importance of collaboration
Last year saw the introduction of integrated care systems (ICSs) across the UK. ICSs should help us to integrate services effectively and drive collaboration between service providers, such as care homes, GPs and hospitals. Collaboration across sectors is essential to keep people healthy, reduce inequalities, enhance productivity and value, and support economic and social development. ICSs will play a key role in enabling us to remove silos between health and social care providers, while increased collaboration will reduce duplication and fragmentation, disseminate best practice and progress in technology.
Through collaboration we can create a truly joined up approach where we listen to citizens, understand their everyday needs and work together to bridge gaps in our services. Building on ongoing collaborations will see a system begin to emerge that is better connected and user focused. The latest generation of digital solutions broaden the circle of care to engage families, friends and communities, and promote services that are connected and data-driven.
Strong relationships between health and care providers and end users is vital to ensure users feel both respected and protected. This in turn can lead to clearer communication, giving care providers the opportunity to deliver care that is targeted to the requirements of individuals.
The workplace and a cultural shift
The digital transition is an opportunity to create a clearer and consistent approach to care delivery. Collaboration is essential but to encourage this, a cultural shift must take place. While technology has sometimes previously been viewed as an additional aspect of service delivery, embedding digital solutions into services will contribute to the successful transformation of existing care models, and provide more intelligent insight to improve health outcomes and protect the dignity of vulnerable people.
Increasing system capacity and capability, as well as providing a foundation for future technological advancement, will see health and care services more able to effectively meet the changing demands of the population. There are compelling benefits for all stakeholders when it comes to technology, particularly from an economic and operational perspective. By driving education within the health and care landscape and building on an already shifting culture, we’ll see more professionals become open to the idea of using technology and transfer their skills, knowledge and experience to the people they care for, to create a digitised world.
A dignified future for care users
As people live longer, increased pressure is put on our care services. Technology has the ability to aid the management of this and potentially reduce pressure points. If successful and integrated digital services for citizens can be realised, the benefits flow will through the health and care system. If we get our approach right, citizens can live independently for longer and have more choice and control.
As we look to a more digital future, we must consider how we can best harness the power of the connected world and the value that can come from technology solutions. By committing to investment in more technological solutions, we will reform our services, improve outcomes and place users at the centre of care to protect their dignity.
BEAMS banishes alarm fatigue at Sheffield Children’s
By Integrated Care Journal and Gabriel Blaazer
On a recent visit to Sheffield Children’s Hospital, ICJ found out about the benefits that BEAMS – the world’s first acoustic bedside equipment alarm monitoring system – has had on patient safety and staff workload.
Hospital staff are rightly keen to have all the tools at their disposal to be able to respond to urgent situations on wards and prioritise patient care effectively.
Bedside alarms are a case in point. They improve patient care, reduce stress for staff, and produce better outcomes for the wider health system. When Sheffield Children’s NHS Foundation Trust approached TBG Solutions in 2018, the trust was soon to be opening a new hospital wing, housing wards up to two times bigger than previously existed. The wing would also feature a higher percentage of single bedrooms than there were in the past.
While a boon to patient privacy and dignity, and better for infection control, the shift presented Sheffield Children’s then Medical Director, Professor Derek Burke, with a conundrum; how to preserve patient safety and ensure that alarms were heard and responded to when patients were behind closed doors?
Founded in 1876, Sheffield Children’s is one of only three stand-alone specialist children’s hospitals in the UK, primarily covering Sheffield and South Yorkshire but also offering specialist services to children from across the UK and internationally.
ICJ recently visited Sheffield Children’s to speak to the Matron for Medicine Care Group, Joanne Reid-Roberts, about the impact that BEAMS has had on nursing practice and patient safety in the new wing. We also asked Paul Rawlinson, Managing Director of TBG Solutions and sister company Tutum Medical, to speak to ICJ about the inception, design and roll-out of BEAMS, and about his vision for the future of BEAMS.
Why BEAMS?
Although not a medical device company, TBG Solutions is no stranger to highly complex technology, operating as a provider of testing, measurement, and control solutions to the aerospace, automotive, defence, medical and energy sectors. As such, they were well placed to take up Sheffield Children’s challenge, which Paul Rawlinson explains: “Most monitoring systems require central monitoring, and every piece of equipment needs to be plugged in to power and ethernet. If you’ve got eight or nine different pieces from different manufacturers, your only option is to have eight or nine central monitoring systems.
“Alternatively, you can go to a third party who will give you one interface, but you need to have the software library to mimic the instrument or touchscreen. If you need to add a new piece of equipment and there’s no software library from these third parties, then there is no interface. These solutions are also expensive,” adds Paul.
After a period of close consultation between Sheffield Children’s and TBG Solutions, the latter “concluded that for the best possible benefit to patient safety, you need a nurse in each room – which of course, you’re not going to get – but putting the ear of a nurse in the room is the next best thing.”
BEAMS utilises its own Wi-Fi mesh network, removing the need to interface with existing hospital infrastructure.
From this brief, BEAMS – and Tutum Medical – were born. BEAMS works by picking up and identifying tonal noises emitted by alarms, routing alerts to a central monitoring system through its own Wi-Fi mesh network – removing the need to interface with existing hospital infrastructure.
“Not only can it do this in an environment that might have a radio or TV on,” maintains Paul, “it can also identify what the equipment is doing. It could be a ventilator’s high priority alarm, and BEAMS can provide this detailed data. And so, if a nurse has four or five alarms going off, such as a ventilator alarm and an end-of-infusion alarm for an IV drip, they are able to prioritise which one to address first.”
Fewer alarms, safer patients
Following a clinical trial, designed to make it possible to compare alarm response times before and after the installation of BEAMS, the system was found to produce an 84 per cent reduction in the maximum alarm response time, and a 74 per cent average alarm response time. The system was subsequently installed into 70 single-occupancy rooms, and it has fast become a vital fixture for the Matron, Joanne Reid-Roberts.
Joanne tells Hospital Times that she “couldn’t imagine being on the wards without it”. She credits BEAMS with inducing a “calmer, and more relaxed atmosphere” on the wing, and helping to address the harmful consequences of alarm fatigue.
Studies have shown that in paediatric wards, up to 99 per cent of clinical alarms are either false or clinically insignificant (such as a battery needing to be changed) and do not warrant clinical intervention. Research also shows the consequences of this dynamic – alarm fatigue – which arises when alarms are so numerous (and often inconsequential) that they blend into the background and are missed.
BEAMS addresses alarm fatigue by helping to reduce the number of alarms sounding at any one time, relaying alarm information in a details spoken notification and making it more likely that any one will be picked up. The statistics appear to back this up; alarm response times at Sheffield Children’s have been cut by an average of 90 per cent, down to just 40 seconds.
“We wouldn’t be able to function without it.”
These efficiency savings add up, bringing benefits to patient safety. “If a patient is on intravenous antibiotics,” Joanne illustrates, “BEAMS alerts us to say that the infusion has ended. If we missed that alert even for 30 minutes previously, what should have taken an hour would end up taking an hour and a half. It may sound small, but this can have a big impact on recovery.”
The second generation of BEAMS, currently in use at Sheffield Children’s and at Leeds Children’s Hospital, communicates the precise nature and severity of alarms, enabling the efficient delegation of tasks and saving precious clinical resource. It can now be instantly established whether an alarm requires the intervention of clinical staff or a support worker, “which has really improved the utilisation of our time,” Joanne adds.
Another important aspect of BEAMS is its reporting mechanism, which allows ward managers to see week-to-week reports detailing the number, location and nature of alarms, and response times, allowing them to pinpoint exactly where improvements are needed. Joanne is under no illusions that such comprehensive data reporting strengthened the impact of the BEAMS pilot, allowing them to demonstrate proof of concept and gain buy-in from the trust’s procurement and finance managers.
Importantly, and key for the workforce, Joanne is certain that BEAMS “has taken away many aspects of stress for staff. We no longer have to walk corridors just in case there is an alarm going off. It’s simple when you think about it, but we wouldn’t be able to function without it.”
Peace of mind for patients and carers
Having a loved one in hospital can be a troubling and anxious experience for anybody, not least when the patient is a child. In paediatrics, mere seconds can prove the difference between life and death – under certain conditions, children can reach an emergency condition faster than adults. This is often the case with respiratory conditions, where the smaller relative size of children’s airways can lead to greater difficulty with breathing than in adults.
Joanne Reid-Roberts, Matron for Medicine Care Group, Sheffield Children’s Hospital (L) and Paul Rawlinson, Managing Director, TBG Solutions and Tutum Medical (R)
While BEAMS has been successful in reducing average alarm response times, feedback from patients, parents and carers at Sheffield Children’s shows the reassuring effect it can also have. “It gives parents peace of mind,” Joanne relates. “It used to be normal that parents complained that alarms weren’t being addressed in a timely manner but that almost never happens anymore.”
She finds that most parents do not like to press the nurse call alarm for fear of wasting their time, yet are also fearful of what might happen if they are not at their child’s bedside. But, “BEAMS gives parents the confidence to know that the nurses will respond to their child’s needs if they are not there, and patients feel reassured because they know that somebody is coming,” a factor that can be important for recovery, explains Joanne.
Just the beginning for BEAMS
Joanne was full of praise for the manner in which Tutum Medical supported Sheffield Children’s throughout the trialling of BEAMS, recalling how easy it was to contact the company, and the fact that “they listened to our feedback and changed the product” according to need.
Why has BEAMS mostly been taken up in paediatric settings thus far? “It just so happened to be Sheffield Children’s who first wanted to trial BEAMS,” Paul says, “and Leeds like to look at what other children’s hospitals are doing.” Looking to the future, however, Paul hopes to see BEAMS deployed in other, non-paediatric settings (citing its particular utility for respiratory wards), and trials are indeed underway at a number of hospitals in England. According to Joanne, “there is no reason why BEAMS couldn’t go into adult services, as they will experience the same issues as us and will probably have less staff than we do.”
At Sheffield Children’s at least, the results are in; BEAMS is one of the tools that helps healthcare staff to provide the best possible care for their patients.