Labour urged to support and protect NHS’ temporary healthcare workforce
By Integrated Care Journal
The UK’s temporary healthcare workforce needs championing and protecting, suggests the Recruitment and Employment Confederation (REC), as it launches its people-first ‘Voice of the Worker’ campaign.
The Recruitment and Employment Confederation (REC) is urging the government to champion the UK’s temporary healthcare workforce, with the launch of it’s people-first ‘Voice of the Worker’ campaign.
The campaign comes as the new government is pushing on with its Employment Rights Bill within its first 100 days in power.
The move has sparked robust debate regarding recruitment and employment, because highly regulated agency work already offers employment rights and in-work progression. There are fears that anticipated changes to employment rules could put the temporary worker market at risk.
Further, the new government’s launch of Skills England will also create more opportunities for temporary and contract workers to upskill as the Apprenticeship Levy is reformed. Although not confirmed, the government is expected to expand the Apprenticeship Levy into a ‘Growth and Skills Levy’, allowing companies to use 50 per cent of their levy contributions to fund training via routes other than apprenticeships.
Temporary healthcare work is key in helping the NHS deal with disparate and fluctuating demand, and with the right regulations in place, enable workers greater flexibility in work and control over their work-life balance.
Neil Carberry, REC Chief Executive, said: “Flexibility at work is something to feel optimistic about. It is working for millions of people. Individual choice and employers’ need for a versatile workforce can be brought together to deliver better careers and higher productivity. The government must ensure new rules support temps and that means having a real understanding of their lives.”
REC’s campaign aims to show how and why temping can work for many individuals by placing the real-life stories of temps, including those working in healthcare, at its heart. The campaign urges government, employers and unions to collaborate more closely to support the UK’s growing temporary workforce.
For the campaign, REC commissioned Whitestone Insight to interview 520 temp agency workers across different sectors – not just health – in Britain in June 2024, to hear their thoughts about agency work and why it matters to them. Polling found:
Almost eight in 10 temp agency workers (79 per cent) said their work provides an important need for flexibility.
More than two thirds of temp agency workers (68 per cent) said that their work provides a greater work-life balance.
More than half of temp agency workers (53 per cent) believed that this is the right kind of role for their current stage in life – an active choice.
REC says it hopes its ‘Voice of the Worker’ campaign will prompt far more discussion about reform of the public sector, with public services clearly struggling with demand. Temporary workers are critical in enabling the NHS to deliver services, helping to retain skilled people in the workforce and provide solutions to NHS trusts. But NHS policies for frameworks and banks have reduced the attraction of working for the NHS for medical staff – and forced trusts to use more and more emergency shifts. By reforming frameworks, their rates and the approach taken to permanent staffing, the new government could reduce costs and get better results for patients and the Treasury. But a proper partnership is needed to achieve this, the REC argues.
Neil Carberry added: “Government has repeatedly made the same mistakes in NHS staffing for almost a decade – trying to pay agency staff less year-on-year than they pay substantive staff. And pretending that Banks are cheaper to the exchequer. The result of this is that there are more emergency shifts as medics reject shifts, and spending overall has gone up. Moving on from demonising agency nurses and doctors and other clinicians – and the agencies that supply them – and working in partnership with the sector on a new approach to procurement will give the new government a unique opportunity to build a sustainable supply of short-term staff, at high quality and value for both patient and taxpayer.
“Good and lasting workforce changes that are effective for workers and employers, happen when employers and government work together to determine what works for everyone. Our case studies show the difference talented agency and contract staff are already making in our health service.”
This autumn, the REC will highlight video and written case studies of temporary workers, in which they explain the reasons for wanting flexibility and the benefits of temp working, across a variety of sectors.
Labour needs a preventative health strategy to transform public health
By Tina Woods
Business for Health Founder and CEO, Tina Woods, discusses the crucial role that business can play in improving the nation’s health, and calls on the Labour government to adopt a shift towards evidence-based prevention.
As the new Labour Government enters its early stages in power, it is increasingly clear that the party has inherited a sick workforce, rising levels of economic inactivity and unsustainable pressure on the NHS.
Tackling our current broken health system requires a long-term, multifaceted approach that shifts the UK’s societal attitude from reliance on the NHS to a culture of prevention. Going forward, creating a comprehensive preventative health strategy should be Labour’s focus.
Laying the foundations for a ‘prevention first’ revolution
Labour’s Health Mission in their manifesto states the aim to “deliver a ‘prevention first’ revolution”, and with the right partners and a clear strategy, this vision can become a reality.
While the ambition to halve heart attacks and strokes, create a smoke-free generation, and reduce health inequality are commendable, translating these goals into tangible policy and action will be crucial.
A preventative health strategy must go beyond individual behaviour change and address the wider determinants of health. This includes creating healthy environments, reforming the food system, and ensuring good work and housing for all. Crucially, it requires coordinated action across government departments, and wider businesses.
Easing pressures on hospitals
The UK’s poor public health is placing immense pressure on the NHS, resulting in many hospitals having far too many patients, with far too long waiting lists.
Despite over 95 per cent of the NHS budget being spent on treatment, with little ring-fenced for prevention, preventable conditions like obesity, heart disease, and lung cancer account for a significant proportion of hospital admissions and healthcare costs.
The government should set a target to allocate a specific percentage of the total health budget to evidence-based prevention programmes within 5 years, rising by 2030. Moving more pathways of care into community health will alleviate pressure on hospitals and create a more sustainable healthcare system. To support in setting and managing these targets, Business for Health has partnered with the Office for National Statistics (ONS) to deliver an enhanced ONS Health Index which will be vital in tracking against the Government’s health and wellbeing plans.
Business is essential in prevention
Alongside the NHS, businesses also have a crucial role to play in this agenda, and the Labour government must work to cultivate meaningful partnerships with the private sector.
By creating incentives and frameworks for improving health, small and medium-sized enterprises can be encouraged to do more; exploring legislation, such as making workplace health reporting mandatory for larger companies, is another driver. To support businesses in creating these strategies, the next iteration of the ONS Health Index will include additional data and tools which businesses will be able to use to understand the health of their workforce and customers better.
Looking ahead, business leaders and employees alike will be eager to see legislation and clear targets from the Labour government, accompanied by investment to support a prevention economy. Businesses are essential partners in creating healthy workplaces, promoting active lifestyles, and tackling issues like obesity and mental ill-health.
A prescription for the future
Ultimately, Labour’s health agenda must move beyond short-term fixes and invest in long-term system change. This will require bold political leadership, a willingness to tackle vested interests, and a collaborative, cross-party approach bringing together government, business, communities and individuals. Only then can we build a healthier, more prosperous future for the nation.
ONS and Business for Health partner to enhance the ONS Health Index
By Integrated Care Journal
The Index will capture a wide range of health inputs, including wider societal and economic determinants, to fill the evidence gap on the interplay between health, business and work and encourage businesses to take responsibility for their impacts on health.
Business for Health and the Office for National Statistics (ONS) have announced a collaboration to develop the next iteration of the ONS Health Index – a tool to support businesses, local authorities, integrated care boards, and government on decisions to ‘invest for health and economic growth’ and inform the Treasury on the economic case for prevention.
The ONS Health Index, last published in summer 2023, measures health in its broadest terms and seeks to understand how it is changing over time. It tracks health in clinical terms (i.e. the prevalence of certain conditions), but also looks at the wider social, economic and environmental drivers of health, together with personal circumstances.
Building on these measures, the enhanced ONS Health Index will include additional data and tools relevant to businesses and their practices. These could range from capturing direct health impacts on employees and customers, to environmental impacts of a company’s products. This will increase the understanding of the interplay between health and business and work life and fill an important evidence gap. For example, it could be used at a local level to help measure corporate progress against key health and wellbeing aims.
More broadly, the additional business themed metrics will inform strategies around the link between health and wellbeing and workforce productivity, and the role of health within the Environmental Social and Governance discussion.
Business for Health, a business-led social venture, in collaboration with Lane Clark & Peacock (LCP), have identified demand from businesses and organisations for the continuation and enhancement of this tool to define their role in the economy and wider society.
They will engage with businesses to develop the next iteration of the Index that provides high-value data on the health and well-being of the nation, including the workforce. One of the key goals will be to encourage businesses to understand and take responsibility for their impacts on health. To this end, the next iteration of the ONS Health Index will seek to bring businesses into its core audiences and provide health-relevant data to the public that measures the impact of businesses on population health.
These additional data will aim to highlight key determinants influencing employee health, and in doing so, inform business decision-making and support organisational and corporate culture with health at its core.
With the UK’s general population currently facing significant health challenges, leading to long term economic inactivity and pressures on the health system, the enhancement of the ONS Health Index will enable focus on facilitating system change to improve health and wealth outcomes. This is vital for enhancing the health and economic resilience of the nation.
Tina Woods, CEO and Founder of Business for Health, said: “There is a clear need from businesses to receive better data on the role of health within wider workforce planning. The link between corporate culture and individuals’ physical and mental wellbeing is irrefutable and our role on the new ONS Health Index will act as a crucial tool in understanding how businesses can improve, report and measure their impact on health linked to economic growth.”
Lord Bethell, Former Health and Innovation Minister and Chair of Business for Health, said: “We are delighted to be working with the ONS and LCP to develop the next iteration of the ONS Health Index, which will differentiate itself by allowing companies to understand and define their social purpose alongside measuring their economic contribution.”
Jonathan Pearson Stuttard, Head of Health Analytics at LCP, said: “There is a need for employers, businesses and industry partners to work collaboratively with the government to ensure that long-term health challenges are tackled with the urgency that is required.”
Dr James Tucker, Deputy Director of Health, International and Partnerships, Office for National Statistics, said: “The importance of high-quality data to inform strategies and reporting on the health of our workforce is crucial. Working with businesses as core users of the next ONS Health Index will be key in accessing granular data from businesses to feed into the index and provide relevant health data.
Harnessing innovation to deliver medicines optimisation at scale
By Meera Parkash
In this case study, Meera Parkash, Clinical Facilitator, Population Health Management at Optum UK, discusses how medicines optimisation can help free up pharmacy capacity and deliver key improvements to population health management.
At a time when the health system is urgently seeking new ways to cut costs, improve outcomes and reduce health inequalities, there are three areas where medicines optimisation can make an important contribution.
The first is non-adherence to medicines. It is estimated that half of all patients are non-adherent to their prescribed medication, costing the NHS £500m every year. The second concerns over-ordering and over-prescribing. About £300m worth of medicines go unused each year, and around half of this cost is believed to be recoverable. The third and final relates to adverse drug events (ADEs) in primary care, leading to hospital admissions. An estimated 72 per cent of ADEs are avoidable, costing the NHS £100m every year.
Traditionally, clinicians have had to manually search for patients who may need changes to their medication approach. This is extremely time-consuming and may not always be accurate if the data being used is out of date.
Population360® changes this. By integrating fully with clinical systems, it automatically finds and presents opportunities to improve medication safety, non-adherence and cost-effectiveness all in one place – transforming the speed, accuracy and scale of these processes.
Other prescribing decision support tools focus mainly on acute prescriptions and can only process them one patient at a time, whereas Population360 can proactively manage an entire patient population for an ICS at once. It does this by providing safety and adherence alerts for high-risk cases while surfacing lists of patients who may benefit from medication changes.
In light of resourcing pressures on pharmacy teams – which limit the number of structured medication reviews, programme switches, or high-risk drugs monitoring they can undertake using traditional methods – Population360 frees up capacity and helps them cover more ground. This demonstrates that it can be an important enabler for delivering medicines optimisation strategies at scale.
Evidence of success
Working with a GP practice covering 10,000 patients, Population360 flagged opportunities to save £82,376 through simple medication switches and recommended 1,171 patients for an adherence or safety intervention over a three-month period.
Based on these, a single pharmacy technician successfully reviewed 16 patients in less than 30 minutes, actively booking tests for 14 patients and initiating a patient consultation and de-prescribe for another.
Another pharmacist reviewed all female patients prescribed sodium valproate based on a targeted clinical rule. The pharmacist contacted patients, reminding them to follow up with their consultant to ensure Annual Risk Acknowledgement Forms were up to date (most of which were not) and contraception was in place.
Both examples demonstrate clinicians working proactively, supporting structured medication reviews, and closing important gaps in care.
The lead pharmacist at the GP surgery said: “It (Population360) gives us these patients very, very quickly and we can review them and take appropriate action – some of these patients are hard to reach people which is also an advantage.”
To see how Optum advances medicines optimisation (MO) and to learn more about proactive prescribing at scale, please click here.
Vic Townshend: ‘Whole person’ understanding is reliant on intelligence-informed decisions
By Ameneh Saatchi
Vic Townshend, Programme Director for Population Health Management (PHM) at Lincolnshire ICS, speaks with Public Policy Projects’ Ameneh Saatchi.
Building capacity and capability for population health management (PHM) is perhaps one of the single most significant enablers of truly integrated care and ambitions for England’s 42 integrated care systems (ICSs). But while every ICS will place significant priority on establishing comprehensive PHM, immediate service pressures and restricted resources have led to mixed results across the country.
In Lincolnshire, the ICS has established the Lincolnshire ICS Population Health Management Programme, which uses a ground-breaking person-level linked dataset, recognised as one of the most extensive in the country. The Lincolnshire Joined Intelligence Dataset covers 100 per cent of the local GP registered population. It encompasses a range of data sources, including primary and secondary care, adult social care, elective waiting lists, deprivation indices, social vulnerability and isolation measures from the Office for National Statistics, Census data, and community asset registers.
This initiative originated with the NHS England sponsored Population Health Management development programme, which allowed for the system to test what PHM offered and supported the first linked dataset to be created for a proportion of the county’s population. Other systems do have linked datasets, but there are none currently known that have the same extent of sources and population coverage.
“I worked closely with the Director of Intelligence and Analytics [Katy Hardwick],” says Vic, explaining that the team entered a partnership with Optum UK, to build the first ever linked data set in 2019, which initially covered about 30 per cent of the population. “This gave us data joined at the personal level, allowing us to see a person’s journey through health and ill-health and how they interacted with services across Lincolnshire to support their needs.”
The data science tool employed by Lincolnshire ICS focuses primarily on measuring health and care utilisation across different contexts, emphasising unit of activity and associated indicative costs. Traditional metrics, such as length of stay are incorporated, offering a comprehensive view of resource utilisation. Moreover, the tool’s versatility allows for customised presentations of intelligence, enabling users to tailor insights to their specific needs. Insights into health inequalities are facilitated by comparing cohorts of individuals, shedding light on variation in outcomes and contributing to high quality decision-making.
In addition to traditional metrics and the sources listed above, the Lincolnshire dataset also encompasses prescribing and medicines utilisation data, facilitating a holistic, system-wide understanding of health and care activities, service utilisation and outcomes. The dataset captures activity from all community, acute and mental health services, drawing from data recorded in trusts’ National Minimum Data Sets. This ensures seamless integration of data, irrespective of where individuals receive treatment – even if that treatment is outside of Lincolnshire ICS.
In healthcare, intelligence-informed decision-making stands as a crucial factor in navigating complex systems effectively. Vic emphasises the importance of this approach, highlighting how linked data allows for a comprehensive understanding of the impact of interventions across healthcare settings.
“The linked data set allows us to identify where opportunities are for intervention and change [and] where we’re doing well,” Vic explains. “What it doesn’t tell us is what we should do with it, but it starts to prompt leaders to ask the right questions… there’s nobody in our system that just has diabetes, which brings into question why we are providing services for diabetics in silo when they have more than one long-term condition and are subject to many other wider determinants of health, such as deprivation.”
This enhanced visibility helps stakeholders to identify both direct and indirect benefits and drawbacks of interventions, leading to better-informed decisions.
“The linked data set allows intelligence-informed decision-making, [meaning] we can now see the impact of our actions across our organisational borders and identify indirect benefits and disbenefits. So, we can track how changes in general practice are improving outcomes across other services, or vice versa.”
The inclusion of indicative costing within the linked data set also provides insights into resource allocation and workforce interactions. This allows for a more subtle understanding of how resources are utilised within the healthcare system, facilitating efficient resource management and optimisation.
Evaluation plays a pivotal role in assessing the effectiveness of interventions and changes in healthcare delivery. Vic underscores the necessity of robust evaluation, encompassing both qualitative and quantitative measures. However, Vic also acknowledges the challenge of maintaining the usability of the linked dataset while incorporating qualitative elements, emphasising the need for flexibility in its development and usage.
“Intelligence-informed decision-making becomes your North Star; you’re all following the same intelligence that steers in the same direction, wherever you work within the system. It has allowed us to robustly evaluate qualitative and quantitative outcomes, so it’s not just about what we can measure in the dataset, but working with personalisation, understanding what outcomes are important to people.”
Overall, the linked data set serves as a valuable tool for identifying opportunities for intervention and making informed decisions that lead to improved outcomes for patient and wider health system.
Vic’s journey into PHM stems from a diverse background, transitioning from the RAF as a meteorology officer, to a decade in general management in healthcare, to change management in complex systems. A keen interest in data analysis has been the nexus between various positions throughout her career.
More recently, Vic has begun addressing performance improvement challenges in healthcare, focusing on the interconnectedness of prescribing practices and care pathways. As Director of the Population Health Management programme in Lincolnshire ICS, she emphasises the need for comprehensive, intelligence-informed decision-making in healthcare leadership, seeing it as pivotal for driving systemic change and improving outcomes. For Vic, PHM represents a transformative tool with the potential to fundamentally change healthcare systems and improve outcomes for all.
The inequality challenge
Intelligence Leads and Chief Analysts working within ICSs will have increasingly important roles in navigating the complexities of health inequalities. Such roles require skill sets that can play a crucial role in generating intelligence to inform various inquiries regarding clinical care outcomes, health and wellbeing, and wider determinants of health. By fostering relationships with them, healthcare professionals can gain access to previously untapped data sets or intelligence that can address longstanding questions or concerns.
While population health itself is not a new concept, the current level of focus being placed on PHM requires significant new infrastructure support, the need for which may not yet be universally recognised within individual health systems. Therefore, she advises initiating discussions with intelligence teams to explore existing available data and infrastructure.
Vic stresses the importance of incorporating intelligence specialists or analysts into discussions alongside clinicians and decision-makers. This tripartite arrangement ensures that data-driven insights inform decision-making processes effectively, leading to more informed and impactful strategy.
Wound care from the lens of population health management
Vic underscores several key priorities essential for improving Wound Care outcomes:
Consistent documentation on electronic systems
Vic emphasises the importance of developing consistent documentation of wound care activities on electronic systems across frontline services and at strategic level. This consistency ensures accurate data collection that is crucial, not only for clinical records, but also for evidence-based decision-making and outcome evaluation. This is something Lincolnshire ICS will be working to develop further, as Vic identifies a challenge in ensuring consistency across local teams to capture all necessary data for wound care. Addressing this challenge is fundamental for systems to improve efficiency and workforce challenges in the community but may require additional resources and strategies to improve documentation practices.
Personalised care approach
Vic discusses the need to personalise wound care, highlighting that different individuals may require different approaches based on their specific needs and preferences for self-care. This personalised approach ensures that care is tailored to everyone’s circumstances, improving overall outcomes.
Training and applying best practices
Ensuring that clinical teams involved in wound care across various organisations are trained in, and consistently utilise, best practices. This helps standardise care delivery with the aim of adhering to established standards and protocols and improves overall quality of care.
Evaluation and continuous improvement
Establishing mechanisms for evaluating the effectiveness of changes made in wound care practices and processes. This iterative approach to improvement allows for ongoing refinement and optimisation of care delivery. This involves identifying what works, what doesn’t, and adjusting accordingly to continuously improve care delivery.
Communication and engagement
Vic underscores the necessity of effective communication and engagement strategies to drive change and improve outcomes for individuals. Engaging the workforce and the population is essential for raising awareness about available treatments and promoting better understanding of wound care options.
Extending pharmacy services – the pros and cons
Vic acknowledges the potential of community pharmacists in wound care as they are in the heart of communities, close to the patients, and can have a further role in early intervention. But she raises concerns about the sustainability and consistency of extending their roles. Vic highlights challenges such as increased workload, inconsistent sign-up to extended services, and competing priorities within the pharmacy profession.
Vic also provides recommendations to apply population health management techniques to diabetes care for comprehensive support
Vic asserts the need to shift away from treating diabetes as a standalone condition and to instead adopt a holistic approach that addresses individuals’ overall health needs. She advocates for integrated care models that offer comprehensive support, ensuring that individuals receive assistance beyond diabetes management alone. This approach aims to improve overall health outcomes and reduce the likelihood of complications associated with diabetes, such as leg ulcers and amputations.
Empowering prevention strategies
Furthermore, Vic highlights the importance of prevention strategies in combating diabetes. She stresses the need for a cohesive and proactive focus on prevention, encompassing primary, secondary, and tertiary prevention efforts. By investing in preventive measures and proactive interventions, such as health and wellbeing initiatives and collaborations with voluntary sectors, individuals can be empowered to manage their diabetes effectively and avoid frequent visits to healthcare providers.
Personalised care: addressing individual needs
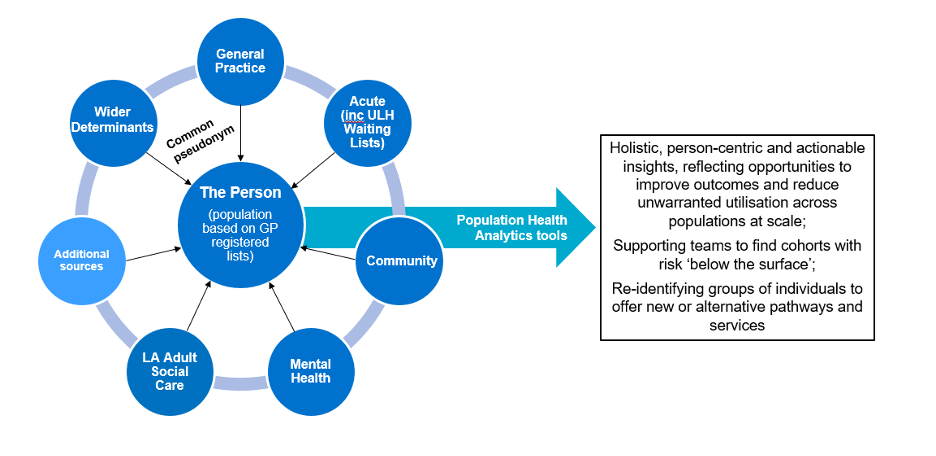
Lastly, Vic underscores the significance of a personalised approach to diabetes care. She advocates for a strengths-based conversation that empowers individuals to take charge of their health while ensuring that healthcare systems meet their personal needs. By tailoring care plans to individual circumstances and preferences, healthcare providers can address inequalities and deliver more effective and meaningful support. This collaborative approach involves engaging individuals in decision-making processes and considering factors such as housing, employment, and social support to create sustainable and equitable healthcare services. Figure 1 below demonstrates how population health analytics tools can improve outcomes and efficiency.
Figure 1: Population Health Management Tools, the bridge between the person and the system strategy (click to englarge)
Conclusion
Vic emphasises the critical need for consistent documentation of wound care activities across all levels of healthcare delivery. This ensures accurate data collection, essential for evidence-based decision-making and evaluating outcomes. Additionally, she underscores the importance of a personalised care approach, recognising that individual needs may vary significantly. Training in best practices, continuous evaluation, and effective communication and engagement strategies are identified as key priorities to drive improvements in wound care delivery.
However, a significant challenge arises from the inconsistent capture of data by community nurses. This gap in documentation poses a barrier to comprehensive data analysis and evidence-based decision-making. Addressing this challenge will require focused efforts to improve documentation practices and ensure that all relevant data are captured accurately. By prioritising efforts to enhance data collection consistency, healthcare providers can strengthen the foundation for effective wound care delivery and evaluation.
What’s next?
Diabetes and wound care are the second and third highest expense to the health system respectively, and impact millions of people in the United Kingdom. Public Policy Projects is launching the second part of its Diabetes Care programme in the autumn of 2024 called ‘Holistic approaches to diabetes care – treating the whole patient’. Vic Townshend will be presenting on 2nd December, in London at the PPP Wound Care conference.
Contact Ameneh Saatchi, Director of Market Access for Diabetes and Wound Care, should you wish to learn more about these programmes: ameneh.saatchi@publicpolicyprojects.com
Developing a life sciences superpower – how the General Election will shape support for the medical technology and pharmaceutical sectors
By Seb Phillips, Senior Account Manager, PLMR Healthcomms
The life sciences industry’s contribution to the UK economy cannot be understated. One in every 121 employed people in the UK work in the sector, which is worth more than £90 billion to the UK economy, and is responsible for world-leading vaccines, robots, medicines and scanners.
Medical technology and pharmaceutical solutions cover almost all medical diagnosis and treatment, and share a mission to improve health outcomes, right the way through from prevention to treatment and aftercare. Medical technology covers everything from syringes and sticking plasters to replacement joints and surgical robotics; with pharmaceuticals ranging from paracetamol and over-the-counter cold and flu powder to the world’s most innovative cell and gene therapies and MRNA vaccines.
Medical technologies and pharmaceuticals hold the promise to support both the health and wealth of the nation, but face a range of barriers to enabling the UK to become a life sciences superpower.
Given the importance of the life sciences sector for the national health and economy, and the need for strong local links between the medical technology and pharmaceutical sectors and their future MPs, PLMR Healthcomms has developed the Clusters of Change: Key Electoral Battlegrounds for the Life Sciences Sector insights report.
This report maps the hotspots of the pharmaceutical and medical technology across the country, linking them to the constituencies being fought in the general election. Using the PLMR Candidates Portal the report paints a picture of the MPs who will be representing constituencies with the largest life sciences footprints after the General Election.
Why this election matters for the life sciences sector
While they have their operational differences, both MedTech and pharma function through similar prisms, sharing objectives around regulation, support for innovation, and better adoption pathways through the NHS.
As such, the outcome for this General Election is particularly important to both, with the elected representatives due to take their places in Parliament for the first time – and there will be a large number of new MPs – due to hold some power over how the life sciences landscape is shaped and supported over the next five years.
It is these incoming Parliamentarians who can advocate and help to deliver better regulation, support better adoption, and help drive the Department of Health and Social Care, the Department for Science, Innovation and Technology and the NHS to deliver for patients through better use of the life sciences sector.
The life sciences sector is critical to the long-term prosperity and health of the nation, and it is therefore vital that the incoming Parliamentarians are aware of the impact that they have on their own constituencies and the country as a whole.
Political ambition for the sector
Although both the Conservative and Labour Parties have pledged to make the UK a life sciences superpower, there are differences in how all parties pledge to support the sector. The Conservatives have pledged to drive capital investment; deliver a well-equipped MHRA; support more commercial clinical trials; and deliver a new MedTech pathway that rapidly adopts cost-effective tech.
Labour have promised to launch a new Regulatory Innovation Office; oversee an NHS innovation and adoption Strategy; and support a reduction in the re-evaluation of products shown to be clinically safe and cost effective by NICE.
The smaller parties have also recognised the importance of innovation and life sciences in their approach the NHS; but with both the major parties supporting the sector explicitly, this potential to truly deliver a life sciences superpower is within reach.
To realise that vision, each part of the life sciences sector must ensure that they are building advocates across Parliament, who can promote the benefits of innovation, medical technologies and pharmaceuticals; push Government for action on support for the sector; advocate for policies to ensure there is an appropriate regulatory and adoption landscape to support greater investment, development and deployment of the tools that support the NHS and drive further economic growth.
Thinking afresh as to how to support new ways of thinking and working
The NHS in the UK faces many challenges and at the same time, is guided by an ambition to reform itself to become more geared towards – and responsive to – the needs of the population.
However, there is limited time and space for those who work in the NHS to think creatively about how to respond to these circumstances. The service is extremely busy and it feels as though staff – particularly those responsible for managing and leading – are caught up in a permacrisis, which limits their capacity to think differently and to test out new ways of doing things.
This has led to a fresh corporate imperative for people to embrace systems thinking – and, in practice, to apply the precepts of systems leadership. However, this raises a crucial issue: there are myriad approaches to business leadership these days, as a cursory glance at the groaning shelves of the Airport Academy demonstrates, which can sometimes make systems leadership feel like yet another fad.
As with all fashions, of course, people are sucked into it, partly out of a personal fear of missing out and partly because everyone around them seems to be saying that it’s a trend into which they need to buy.
Current systems thinking
However, approaching the challenges and ambitions of health and social care systemically makes absolute sense. It is a perspective that acknowledges that the whole is greater than the sum of its parts and that a system relies upon meaningful connectivity between agencies – and individual agents – to maximise that effect.
All of which has led to a busy market of workshops, courses, and programmes that aim to induct people into systems thinking. However, these tend to take place at a distance from the practicalities of what it is like to make sense of systemic working in practice and to navigate it in a positive fashion.
There is a paradox at the heart of this. The busyness that managers and leaders in the NHS face at this time denies them the headspace to think systemically in the context of their systems. They are frantically doggy paddling in order to keep their heads above water, which prevents them from learning in the pool the swimming strokes that would make the situation smoother and easier.
On the other hand, there is an effort to teach people about systems – but this is taking place away from the practicalities of work in a quite abstract fashion. It’s as if people are stepping out of the pool to sit in a classroom to be shown the theory behind other swim strokes that might support them better in the water.
Crisis and leadership
Why is proximity to practice so important in this instance? Primarily because our organisational focus in most instances is on structure: we focus constantly on the scaffolding that envelops the work that we are asked to do. Yet the latter occurs systemically, with a passing relationship to the structure but in many ways independently of it.
Importantly, it is arguable that recent experience shows us that systems become apparent, and we are better able to acknowledge their presence, at times when we face crisis. There are examples cited by Rhiannon Firth in her book Disaster Anarchy – for instance, the aftermath of Hurricane Sandy in the US – where disasters outstripped the state’s capacity to respond, due to its structural emphasis, but out of which arose mutual aid arrangements, which were systemic responses.
A clinician with whom I spoke at the peak of the Covid 19 pandemic explained that it used to take her at least three days to organise a patient transfer. Invariably, to action it, she would need to involve people above her in the hierarchy. However, with the arrival of coronavirus, she found it necessary to step into leadership – and she quickly found that she could network with opposite numbers in other agencies at a grassroots level…and suddenly transfers could be achieved in around half a day.
This is important learning about how structures can often constrain innovative approaches to getting things done – and that an experience of crisis can create a tendency for systemic working to come to the fore. The challenge, however, is to preserve that learning about systems that arises out of difficult practice, when organisational elasticity tends to see things snap back into place, with bureaucratic structure reasserting itself.
Learning about systems from systems
Over the course of the past six months, I have been in conversation with my colleague and co-thinker Eitan Reich as to how best to help people with systems thinking and practice. This piece is a summary of a longer and more detailed white paper, which can be accessed HERE.
We have generated several foundational precepts in terms of thinking about this challenge:
Crises tend to cause structures to buckle, which has the positive effect of allowing the systemic underpinning of the workplace to become more apparent – and hence more widely applicable.
Seeking to “teach” people about systems at a distance from the systems is too abstract an approach – which will make it feel like an imposition for many leaders.
A useful starting point is to explore people’s recent experiences of crisis, in terms of what they saw happen; what they initially considered doing, and what eventually emerged as a way forward, which may well have been wholly unexpected but needs now to be acknowledged as a different way of working.
Knowingly engaging with the experience of working systemically that arises inadvertently out of extreme circumstances will give people the permission to unlearn traditional leadership thought and practice and to allow a new way of being and doing at work to emerge. For example, the structural mindset requires us to think about directing: to embrace a systemic perspective means that we focus instead of finding ways of connecting.
Next steps?
Eitan and I are now extremely eager to identify a couple of partners who are interested to work alongside us in collaboration to continue this exploration and development of a way of helping people to think and practice more systemically in the public sector. If this is something that you might be interested to discuss with us, please drop us a line at radicalod@colefellows.co.uk and we’ll schedule an exploratory call.
Professor Mahendra Patel OBE: Reimagining the role of community pharmacy
By Samantha Semmeling
ICJ recently spoke to Professor Mahendra Patel OBE, leading pharmacy expert and Director for the Centre for Research Equity at the University of Oxford, about his vision for community pharmacy, and how multi-professional collaboration can help the underutilised sector play a key role in the fight against health inequalities.
Public Policy Projects (PPP) is hosting its inaugural Medicines and Care Pathways theatre as part of the Integrated Care Delivery Forum in 2024. The first iteration of the event took place in Birmingham on 9 May where pharmacy professionals joined wider ICS leadership to discuss pharmacy’s contribution to the integrated care agenda.
Professor Mahendra Patel OBE, Director for the Centre for Research Equity at the University of Oxford, and a recently appointed Independent Expert Member to the UK Professional Pharmacy Leadership Advisory Board (UK PPLAB), joined the theatre and highlighted the untapped potential of pharmacy to further contribute to system priorities.
PPP spoke to Mahendra about the current developments in UK pharmacy leadership, multi-professional collaboration, and the role pharmacy professionals can play in reducing health inequalities.
The evolving landscape of pharmacy leadership
In 2023, Mahendra brought his expertise to the UK Commission on Pharmacy Professional Leadership acting as Vice Chair of the Leadership, Policy and Professionalism working group. The Commission’s report concluded that there is ‘insufficient collective leadership’ for pharmacy in the UK, and that pharmacy professionals are generally disengaged from professional leadership bodies (PLBs).
The findings prompted the Commission to recommend the formation by the Department of Health and Social Care of the UK PPLAB, as an independent public body. The board has since appointed its chair and independent expert members, involving representatives from both PLBs and specialist professional groups (SPGs). The board will be implementing the Commission’s recommendations over the next 3 years, including the development of new arrangements for pharmacy leadership in the UK.
On the formation of the UK PPLAB, Mahendra says: “The new leadership board, through its broad-based range of independent experts from across the four nations, provides a robust and meaningful structure to steer the line of professional pharmacy leadership moving forward. Whether that is a royal college with different faculties, or two or three professional bodies under one umbrella – that’s for the UK PPLAB to decide.”
Equally, it’s an exciting time for community pharmacy with emerging new services and the increasingly advanced roles of pharmacists and pharmacy technicians. However, Mahendra warns of potential hurdles when it comes to determining new leadership structures. “There are going to be challenges when uniting all pertinent groups under one umbrella, as they are all resourced differently and to varying extents,” he adds.
Despite this, Mahendra remains excited and optimistic that “representation in this new setting will inspire and instil a breath of fresh air, so that those often disengaged, including a significant number from the community pharmacy sector, will come to believe that there is something in it for everyone across the pharmacy spectrum. The board creates a whole new arena of expertise, voice, and experience, including the patient and public opinion, making it a unique place to strengthen the present and shape the future.”
Multi-professional collaboration – bringing community pharmacy to the table
Beyond the Commission and implementing its recommendations, Mahendra seeks to help further elevate the role of community pharmacy. Using the Sigma conference in South Africa as a platform, he brought together pharmacy, nursing, medical and dentistry leaders from across the four UK nations to discuss the opportunity for multi-professional collaboration in the newly integrated NHS.
Using the implementation of the Pharmacy First service in England as an example, the session underscored the potential for pharmacy to engage in multi-professional collaboration. The service involves collaborative working across pharmacy and general practice to free up GP appointments and demonstrates untapped value in cross-sector working within primary care.
For example, the NHS Chief Dental Officer speaking at the event outlined exciting possibilities for the role of community pharmacy in preventative dental care, especially in reducing the levels of tooth decay in children – an increasingly pressing issue in the UK over recent years.
Mahendra feels that “community pharmacy can play a huge role in the prevention agenda. If we have the prevention agenda better resourced while we are coping with a shortage of dentists, at least we are considering longer-term perspectives.”
He concludes that the professions within healthcare are “united by providing the highest standards of health and care. They are all talking about the same problems but shout about them separately.” He calls for multi-professional collaboration for the benefit of patients and the public to ensure that health and care professionals are communicating to government with one clear voice.
Addressing health inequalities through research equity – the role of pharmacy
Throughout a diverse portfolio career, working to reduce health inequalities, especially in cardiovascular disease and type 2 diabetes, has been an underpinning focus for Mahendra. As Director for the Centre for Research Equity (CfRE), his work aims to target underserved communities and black and ethnic minorities through championing inclusivity and community engagement in health research.
Decades of work have exposed deep inequalities in the health of the UK population. As Mahendra explains, “we have seen the same results time and time again, as far back as the Black Report, two consecutive ten-year Marmot reviews, and most recently with Public Health England’s COVID-19 Report”. The Health Foundation has also pointed out that health inequalities in England are some of the worst among developed countries and are likely to persist without sufficient intervention.
Mahendra argues that engaging communities who are most impacted is essential if we want to prevent this projected widening of inequality. He stresses the role of research equity is a key piece of the puzzle and the role of pharmacy within this is crucially important.
He uses the case of the drug Clopidogrel, an anti-platelet medication used to prevent heart attacks, as an example. “One study showed that those from Bangladeshi or Pakistani origin were 30 per cent less likely to activate the drug once taken. These populations are those more likely to die of heart attacks compared to the white population.”
Garnering evidence which is generalisable across all populations is essential for reducing health inequality. The CfRE aims to achieve this by ensuring representative and more equitable health research.
Where does pharmacy come in?
Nearly 90 per cent of the population in England can access a community pharmacy within a 20-minute walk, and importantly, the ‘Positive Pharmacy Care Law’ exists, mandating that access to pharmacies increases to 100 per cent in areas of greatest deprivation. This makes community pharmacy a uniquely placed asset to engage with communities where health inequalities are most stark.
NHS England is supporting pharmacy to leverage this position. The recently published Report of a UK survey of pharmacy professional’s involvement in research has spearheaded the formation of a Pharmacy Research Advisory Group to implement the report’s recommendations. These include aims to “embed a research culture in pharmacy careers, develop a clinical academic pathway for pharmacy and provide a pipeline of pharmacy research leaders”.
This, in addition to the recognition provided to pharmacy in supporting inclusive research by the CfRE at Oxford University, a world class academic research institution, and the formation of the UK PPLAB, provides a huge boost for the sector.
Mahendra concludes that this recognition “demonstrates the ability of pharmacy to shift the dial of healthcare in many directions, inspiring the next generation of pharmacy professionals as well as those who may not have previously considered it as a career”.
PPP will be hosting the Medicines and Care Pathways theatre at the Integrated Care Delivery Forum in London on 5 November.
The Integrated Care Delivery Forum connects system leaders with on the ground innovators and industry experts to highlight exactly how ICSs are making place based, personalised care a reality. Rather than discuss issues such as health inequalities in broad framing and terminology, the Forum asks local systems leaders and stakeholders to demonstrate exactly how integrated care systems can affect change in key health and care challenges.
For further information about the Delivery Forum theatres, please contact:
EHR roll-outs need strategies to mitigate clinician overload
By Dr Dominic Pimenta, Jasmine Balloch, Dr Ellie Asgari; TORTUS
Clinicians are increasingly subject to cognitive overload, and recent studies suggest that without mitigation strategies in place, poor implementation of EHR systems can exacerbate the problem.
In April, a narrative review paper was published in the JMIR Medical Informatics titled Impact of Electronic Health Record Use on Cognitive Loads and Burnout Among Clinicians. My fellow authors and I applied cognitive load theory to explore the impact that routine EHR use has on clinicians and to suggest how the risk of negative effects could be minimised.
It’s important to preface the discussion of our conclusions by acknowledging that EHR systems are essential for the delivery of efficient, joined-up patient care: they allow for improved communication between clinicians, remote access to clinical records and to a high volume of clinician data for research and audit purposes. Rightly, years of effort and significant investment have led to widespread EHR implementation across the NHS: 87 per cent of primary, secondary and community care staff surveyed by the Health Foundation reported using EHRs as part of their work, and in the 2024 Spring Budget, the Chancellor pledged that they would be rolled out across all NHS Trusts by 2026.
However, only 57 per cent of respondents in the same Health Foundation survey chose EHRs as the technology saving them the most time, and their rapid review of 72 studies about EHRs and related tools identified that 44 per cent found no time savings delivered. This indicates that the potential of EHRs is not yet being fully realised.
As our new review concludes, taking a considered, evidence-informed approach to the design and implementation of EHRs makes all the difference when it comes to unlocking their full potential, while mitigating significant potential risk. Importantly, by acknowledging and proactively addressing the relationship between EHRs and cognitive burden, organisations can successfully reduce rates of clinician burnout and minimise risks to patient safety.
EHRs and cognitive overload: examining the evidence
Cognitive load theory explains that human capacity to process information is limited to a few elements in working memory at any given time. When this capacity is overwhelmed by an excessive quantity of information, the resulting cognitive overload can impair decision making, interfere with mental performance and elevate stress levels. Clinicians are typically at high risk of cognitive overload, as they must navigate complex patient data, integrate new information rapidly, and make critical decisions under pressure on a daily basis. The transition to digital records has compounded this challenge by significantly increasing the volume and complexity of data clinicians must handle during patient care.
Recent studies indicate that poorly designed EHR systems can exacerbate cognitive load. The factors contributing to this include inefficient user interfaces, excessive documentation requirements, and the need to navigate through cumbersome electronic systems to access relevant patient information. In addition, dealing with overly-frequent pop-up notifications has been shown to cause distraction and alert fatigue, both of which can lead to clinicians missing important information and result in poor patient outcomes.
Experiencing regular cognitive overload is a major risk factor for burnout. In 2023, 55 per cent of surveyed NHS workers had experienced burnout in recent years, a condition characterised by emotional exhaustion, demoralisation, and a reduced sense of personal accomplishment, which not only affects individual health professionals but also the quality of care they provide. Although burnout has multiple root causes, addressing the design and implementation of EHRs to reduce the cognitive load they place on clinicians is a necessary and important step towards tackling the rise in burnout cases.
Practical recommendations:
Improving EHR user interfaces: Simplifying the user interface of EHR systems can reduce unnecessary cognitive effort. This involves designing more intuitive menus, reducing the number of steps to complete tasks, and organising patient data more logically.
Streamlining information presentation: Tailoring the presentation of information to minimise extraneous load is crucial. This could mean displaying critical patient data in a summarised form, with the option to expand details as needed, thus preventing information overload.
Reducing documentation burdens: Automating routine data entry and employing natural language processing can decrease the time clinicians spend on documentation. This not only frees up cognitive resources but also allows clinicians to devote more attention to patient care.
Incorporating decision support tools: Advanced decision support tools can aid clinicians by providing contextually relevant information at the point of care, reducing the need for extensive data retrieval and analysis.
Training and support: Continuous training and real-time support can enhance EHR proficiency among clinicians. Tailored training programs that address the specific needs of users can alleviate stress and improve their interaction with the technology.
Importantly, emerging artificial intelligence and machine learning technologies offer promising avenues to manage cognitive load by automating routine tasks and predicting patient risks through advanced analytics. However, the integration of these technologies must be handled carefully to avoid adding to the cognitive burden – evidencing a need for user-friendly design and time-saving clinical integration.
In summary, clinician burnout is complex and has multiple causes – such as overall workload, inflexibility of rostering and organisational culture – which is why it could never be fully eliminated even by the ‘perfect’ design and implementation of an EHR. However, by scientifically assessing the impact of different EHR technologies and models, it becomes possible to paint a more complete picture of how they alleviate or exacerbate burnout. In turn, this understanding can be used to ensure that clinicians are equipped with the best EHR systems –and the best integrated technologies – that improve their efficiency and improve patient outcomes.
The future of occupational therapy and the impact of technology
By Alicia Ridout
Leading occupational therapist, Alicia Ridout, discusses her award-winning work and explores the central role of technology in the future of occupational therapy.
Alicia Ridout, a leading occupational therapist, has recently won the Royal College of Occupational Therapists (RCOT) Tunstall Award for Technology Innovation for her work on the pioneering COG-OT – the Clinical Onboarding Guide for occupational therapists, which she and her team have used to continue their discovery work and to progress the project.
Here, she discusses the importance of technology in occupational therapy and why programmes such as COG-OT are essential for health professional development.
The importance of occupational therapy in wider healthcare
Occupational therapy is essential to the health and care sector and as a sector, we need to ensure that robust systems are put in place to keep up to date with digital competencies and boost confidence to use technology safely, in day-to-day practice. This will help the sector to continue supporting the efforts of the wider health and care landscape to digitise services effectively and improve access for people who need it.
Alicia Ridout, independent occupational therapist and creator of the COG-OT app
Occupational therapy is about working alongside people and their families, helping them achieve their personal goals and essential practical skills, using a holistic approach that respects their strengths and assets. This includes physical, sensory, mental health or communication needs. We see people in a wide range of contexts, people who are experiencing a wide variety of challenges, often for very different reasons.
Occupational therapists’ roles are unique in that we provide services to all age groups, across service boundaries. When it comes to supporting the wider care sector workforce in enabling people to safely access digital tools and services, the sector has always been actively focused on seeking out new technology. COG-OT provides a quick and easy means to access evidence and build competency driven technology skills.
The role of technology in occupational therapy
According to a recent study by RCOT, occupational therapists are facing pressures due to increased demand and vacancies within the industry. This potentially risks leaving people needing assessments, with little or no intervention.
There is a huge opportunity for technology to support people accessing services and occupational therapists, particularly when it comes to prioritising their requirements and influencing technology procurements. Using digital solutions offers the chance to reduce variation in workflows and processes, and also facilitate best clinical practice, streamline access to the right technology, at the right time, and ensure the end user’s experience is high quality.
We launched COG-OT as a web app in 2020, as a proof-of-concept approach to supporting practice development, funded by the Elizabeth Casson Trust. To date, we have won further funding from the Trust to evaluate the tool, as well as funding as part of the RCOT awards twice, in 2021 and 2023, which is crucial for the continued development of this vital resource for occupational therapists.
Why COG-OT has made a difference to the profession
COG-OT supports the profession with guide question sets to stimulate their reasoning about the needs of their service users. It can provide areas of focus and exploration when assessing people who have been referred to their service. This is hugely beneficial to less experienced digital practitioners, as it can help to navigate to the correct technology solution for an individual’s needs and ensure effort invested in the onboarding process is effective. The tool can help therapists by instilling confidence and a consistent but personalised approach to the deployment of technology.
Since the pandemic, digital practice has become increasingly prominent and this is no different in occupational therapy. Digitisation offers its own challenges, but by implementing tools such as COG-OT we are aiming to equip professionals with the digital clinical risk management tools they need for effective practice.
Why investment in technology needs to be prioritised, and how ICSs can support the occupational therapy community
ICSs provide a voice for Allied Health Professions (AHP) via Councils, driving improvement programmes and getting research into practice. The COG-OT team have been working with colleagues in an ICS to surface digital requirements across systems of care and we aim to share this insight widely. Digital confidence is one of many challenges facing AHPs at present, and the wider workforce.
However, as a next step, the sector needs to ensure consistent access to digital solutions, both to support workflows and also speed access to the right technology for users of services and their families. This will ensure that no matter the patient pathway, occupational therapists have easy access to recommended platforms that are of high quality, adhere to regulatory requirements and support clinically driven and collaboratively defined solutions for people in need.
Occupational therapists need to clearly articulate their requirements in this respect. They play a key role in personalised care and ensuring a holistic approach to safe digital deployment at every stage in the care journey – from hospital to community or intermediate care and at home. Digital use at home is different to a hospital environment, and we need to ensure holistic clinical risk assessments are completed.
By integrating safe and high-quality technology into our daily practice, working together with service users and their families and with other health and care professionals, we can pave the way for solutions that really make a difference.