Royal College of Physicians issues stark warning over social care crisis
By Gabriel Blaazer
The Royal College of Physicians is warning that the combination of an ageing population and a lack of NHS workforce planning means the country is risking an unavoidable crisis in social care for older people.
The Royal College of Physicians (RCP) has issued a stark warning that NHS workforce shortages are driving the social care crisis in England and that the NHS is “woefully unprepared to cope with an ageing population.”
New analysis from the RCP shows that there is the equivalent of just one full time geriatrician per 8,031 people over the age of 65 in England. The findings use data from the RCP’s own census of physicians and the Office for National Statistics’ (ONS) population data and demonstrate the extent to which England’s care crisis is only set to grow.
The ONS estimates there will be more than 17 million people aged 65 and above in the UK by 2040, meaning 24 per cent of the population would require geriatric care. Additionally, many of the doctors currently providing geriatric care will, themselves, soon be requiring the same care, and 48 per cent of consultant geriatrics are set to retire within the next 10 years.
Considering these trends, the RCP, along with more than 100 medical organisations, is supporting an amendment to the Health and Social Care Bill requiring the government to publish “regular, independent assessments of the numbers of staff the NHS and social care system need now and in future.” No such data is currently publicly available. The amendment, currently being debated in the House of Lords, was tabled by Baroness Cumberlege and is supported by former NHS England Chief Executive Simon Stevens (now Lord Stevens of Birmingham), is set to be debated in the House of Lords
Responding to the RCP’s warning, Danny Mortimer, Chief Executive of NHS Employers and Deputy Chief Executive of the NHS Confederation, said: “As exhausted NHS staff strive to tackle the enormous treatment backlogs that have resulted from the pandemic, we must not forget about the pressures that our health and social care services face as they work to meet the growing needs of our ageing population.
“To be able to plan effectively for a future workforce, healthcare leaders need clarity in the shape of a clear long-term workforce plan. Sajid Javid’s recent commissioning of a workforce strategy is a very welcome step, but… we would urge the government to accept amendments requiring the health secretary to publish regular, independent assessments of the numbers of staff the NHS and social care system need now and in future.”
The President of the RCP, Andrew Goddard, said: ““I have dedicated my career to working in the NHS – a service that I am fiercely proud of – and yet it scares me to wonder what might happen should I need care as I get older. There simply aren’t enough doctors to go round, not least within geriatrics.
“The workforce crisis we’re facing is largely down to an astonishing lack of planning. All successful organisations rely on long-term workforce planning to meet demand and it’s absurd that we don’t do this for the NHS and social care system. The government needs to accept the amendment put forward by Baroness Cumberlege and make workforce planning a priority.”
Dr Jennifer Burns, President of the British Geriatrics Society, said: “These figures show very clearly the current nationwide shortage of geriatricians – a situation that will only get worse with the predictable rise in the numbers of older people across the UK needing healthcare.
“It is absolutely vital that these fundamental issues around the recruitment, retention, development and support of the workforce are addressed, and that there is a properly-resourced strategy for future needs. The British Geriatrics Society stands with the RCP in strongly supporting the amendment to the Health and Care Bill.”
New white paper seeks to clarify what integration means for patients
By David Duffy
The government has published its eagerly awaited Integration white paper, designed to clarify exactly how integrated services will improve care for patients and end users across England.
The paper outlines a series of priorities for integrated care systems to improve health and care delivery. These include enhancing transparency and choice of care increasing earlier intervention of care, as well as increasing flexibility and developing clearer communications between different service providers and enhancing overall value for the taxpayer.
Commenting on the paper, Prime Minister Boris Johnson said: “These plans will ensure no patient falls between the gap [between services], and that everyone receives the right care in the right place at the right time.”
This sentiment was echoed by Health and Care Secretary Sajid Javid, who said: “Our Integration white paper is part of our wider plans to reform and recover the health and social care system, ensuring everyone gets the treatment and care they need, when and where they need it.”
The Integration white paper follows a day after the NHS published its Elective Care Recovery Plan, outlining how the health service intends to bring down ominous backlog figures and repair waiting times following Covid-19 disruption to services.
Proposals outlined in the recovery plan include a focus on community diagnostics and new approaches to care that will only be possible to deliver through integrated care systems (ICSs). This new white paper seeks to outline how health and care systems will draw on the resources and skills from across NHS and local government to “better meet the needs of communities, reduce wating lists and help level up healthcare across the country”.
Also commenting on the Integration white paper, Mathew Taylor, Chief Executive of the NHS Confederation said: “As these proposals are developed further, it is important that we recognise the differences that exist in local areas including in local relationships. They will need to evolve in their own way if we are to crack this agenda.
“Finally, for integration to work there needs to be joined up thinking across government as well as at local level. Ensuring this will allow local leaders the freedom to work with their communities to identify what will provide the best outcomes for the public.”
Hugh Alderwick, Head of Policy at the Health Foundation, highlighted the importance for adequate funding if these system reforms are to be possible: “Better integration between services is no replacement for properly funding them. The social care system in England is on its knees and central government funding over the coming years is barely enough to meet growing demand for care – let alone expand and improve the system.
“More integration is also little good if there aren’t enough staff to deliver services. Staffing shortages in health and social care are chronic, yet government has no long-term plan to address them.”
Analysis
For those who have been close to the integrated care agenda in recent years, or indeed attended virtually any event around integration, there will be little new insight within this white paper – nor will there be much to disagree with. Health and care integration is not a new concept, and so the broad concepts within the government’s latest paper come with little in the way of new proposals. The paper is more of a clarification on what integrated care seeks to achieve rather than an explanation as to how it will be delivered (the absence of additional funding proposals and clear strategy to address workforce shortages is telling).
Not that the document isn’t useful, public perception and understanding of integrated care is still very poor. Delivering integrated care in practice will be difficult unless this understanding is improved and, to this end, the white paper provides some useful clarifications.
But the timing of the paper is as important as its contents. Building on the recent publication of the Levelling Up white paper and published a day after the NHS elective care recovery plan, the Integration white paper is an attempt to show that the government are looking beyond the acute sector and are serious about “Levelling Up”.
The white paper also comes as the Prime Minister is desperately trying to build some policy momentum and move away from what has been a disastrous period for his premiership. Time will tell whether this series of flagship policy proposals (which will precede a further paper outlining specific plans to address health disparity) will provide the antidote to the partygate scandal.
Key priorities of the white paper:
Better transparency
More personalised care
Earlier intervention
Clear communication
Improved access to social care services through NHS data sharing
The National Care Forum (NCF), the membership organisation for not-for-profit organisations in the care and support sector, has created a range of dedicated resources and information to help social care providers understand, navigate, and improve the integration between health and social care as they prepare for the integrated care systems (ICSs) to go-live on 1 July 2022.
Having now been passed into law, ICSs will be given a statutory underpinning across England as the Health and Care Bill. This partnership model brings together providers and commissioners of NHS services across a specific geographical area with local authorities and other local partners, such as social care and housing, to collectively plan health and care services.
It is a fundamental shift in the way the health and social care system is organised in England – moving away from competition and organisation autonomy to collaboration between health and care organisations to integrate services, reduce health inequalities and improve population health and wellbeing.
The new resources launched by the NCF include:
Definitive, dedicated ICS training: What the social care provider sector can do for the ICS
NCF have partnered with the Housing Associations’ Charitable Trust (HACT) to bring together a dedicated learning and development programme during June and July to support the sector in working with ICSs. The programme aims to enable delegates to engage in long-term partnerships that transform the delivery of health and care, while simultaneously resulting in better integration between social care provider organisations and health. The training will help social care providers:
Understand more about ICSs
Strengthen their understanding of how to engage with their local ICS
Build awareness of the competencies needed to deliver within integrated care settings
Identify partnering opportunities and build credibility
A dedicated and facilitated discussion with NHSEI/DHSC and social care providers as part of a listening exercise on Monday 9th May to understand the challenges and successes of engaging with ICSs. The session will aim to achieve agreement to coproduce a model for engagement with the social care provider sector and to think about where efforts would be most effectively focused. This builds on the collaboration between NCF, NHSEI and DHSC over the last few months to support ICS engagement with the social care sector.
An online ‘one stop shop’ on the NCF websitethat offers a simple overview to ICSs, interactive maps to find out which ICSs operate in any area, key messages to help ICSs understand how social care is central to improving health and care for their local populations and case studies to showcase how engagement can work on the ground to make a difference for people using health and care services.
Vic Rayner OBE, CEO of the National Care Forum said that “the introduction of integrated care systems is a major change to the health and social care system in England and as such it is imperative that the social care sector fully understands and engages with the process of transition to this new model of partnership working.
“We have created these resources to support our colleagues from across the sector to strengthen their understanding, upskill their competencies and build their confidence in identifying partnering opportunities that integrate health and care services while improving peoples’ health and wellbeing.”
If you would like to find out more about the resources available on integrated care systems or to attend the training sessions, please visit the NCF website.
Change to Health and Care Bill: Costly consequences for poorer regions
By Niamh Macdonald
MPs in Yorkshire, the Midlands and the North East should vote down the government’s social care cap amendment to save their poorer constituents from ‘crippling care costs’, warn the Health Foundation and the King’s Fund.
The Health and Care Bill, due to reach final stages in the House of Commons on 25 April, includes an amendment from the government which would mean its social care reforms would offer less protection to poorer people.
According to the Health Foundation and the King’s Fund, people in Yorkshire, the Midlands and North East of England would feel the greatest impact on their protection against high care costs due to the amendment.
In 2021, the government proposed a cap of £86,000 on the lifetime care costs that an individual will have to pay for personal care. However, it also proposed amending the 2014 Care Act to mean that local authority support given to help meet an individual’s care costs would no longer count towards the cap.
This amendment will significantly reduce the benefits of the reforms for people with lower levels of wealth but those with housing wealth of more than £186,000 will be unaffected.
Irrespective of wealth and assets, the amendment will mean everyone will face the same costs. The effects of this are far more severe for those with low to moderate assets, meaning some may be forced to sell their home to finance their care.
A joint Institute for Fiscal Studies (IFS) and Health Foundation report, funded by the Health Foundation, recently assessed the impact of the government’s amendment. It analysed how the amendment would affect people in different regions of the country.
The report found that for people spending ten years in residential care:
People in the North East would spend on average an extra six per cent of their assets on care. This is equivalent to an average increase in contribution of £5,700.
In Yorkshire and Humber people would spend an extra five per cent of their assets, equivalent to £5,300.
In the Midlands it would see an increase in payments worth four per cent of assets, equivalent to £4,600.
These increases compare to two per cent in the South East and one per cent in London, equivalent to £3,800 and £2,800 respectively.
Charles Tallack, Director of Data Analytics at the Health Foundation, said: “The government’s amendment represents a significant watering down of the pledge to protect people from catastrophic care costs.
“At a time when the country is facing the biggest hit to household finances since the 1950s, government should be looking to increase financial protection for poorer households.
“Yet this measure will disproportionally affect people with lower wealth and in poorer areas of the country. This is not levelling up: it’s unfair and a backwards step.”
Sally Warren, Director of Policy at The King’s Fund, said: “The government’s change to the cap on social care costs is expected to save the Treasury money, but that saving comes at the expense of poorer people with lower levels of wealth and assets.
“Many of those people will be wondering why the Prime Minister’s pledge that no one will have to sell their home to pay for their care no longer applies to them, whilst wealthier people are still protected from catastrophic care costs.”
With the conflict in Ukraine raging, care employers are working together to provide opportunities for those displaced to work and find a home in the UK.
Care employers have been working together to understand how they can provide a meaningful employment opportunity for those displaced from Ukraine and other parts of the world and finding a home within the UK.
The National Care Forum (NCF), the leading association of not-for-profit care and support providers, in association with the Care Provider Alliance, have brought together a wide range of partners committed to offering support. This includes expertise from across national and local government, housing, recruitment specialists, legal and immigration experts and regulators.
Employers and partners are working closely with recruitment experts to enable displaced people from Ukraine and other parts of the globe to identify roles within the care sector, direct individuals to localised support and ensure that employers work together to provide the best opportunity for those who wish to work.
While this work progresses, the broader support for people displaced from Ukraine through the Homes for Ukrainians scheme is being clarified. Alongside this, local government has an important role in regards to how local support will work, and specific roles and responsibilities are still emerging. It is imperative that the desire to work is aligned with the need for displaced people to be connected into wider community and pastoral support.
Vic Rayner OBE, CEO of the NCF said: “Like many people affected by the plight of the people of Ukraine, care employers are pulling together to take action to help. The ideas are progressing at pace, and there is a strong desire to do something meaningful to help the people of Ukraine, and others from around the globe who arrive into the UK.
“We are pulling together opportunities for care and support employers to share details of available job vacancies, which we hope will be tied into the broader communications for displaced people. There are many other ways for people to offer support, including support to Ukrainians needing care and support, assistance with vetting and matching, and those who have a housing solution.
“However, there remain significant unanswered questions around regulatory requirements, right to work entitlement, safeguarding, etc. We need the government to work at pace alongside adult social care employers to resolve this. Furthermore, we are working with other partners, to understand how most effectively the sector can be engaged to provide a solution at this moment of crisis.”
More support needed for “fatigued” social care workforce
By Mary Brown
On the 16th March 2022, Public Policy Projects (PPP) hosted an evidence session entitled The Social Care Workforce: Averting a Crisis as part of its report series The Future of Social Care. PPP’s Social Care Network examines the most urgent issues facing social care and presents tangible solutions to address workforce challenges in the sector.
The crisis facing the social care sector is fundamentally a workforce one. The sector itself is a large employer in the UK, employing about 1.54 million people, equivalent to five per cent of the workforce. As one participant noted, “the sector itself is a huge contributor to the economy and to society”. Given that staff pay is the single biggest expenditure faced by care homes, workforce management should be front and centre whenever system finances are being considered.
Even before the pandemic, there were about 112,000 social care vacancies in England, with jobs paying only £8.50 an hour. Following the pandemic, the vacancy figures are assumed to be worse. Key issues driving individuals away from working in the social care sector include low pay, stressful working conditions and a low sense of worth.
A participant of the evidence session emphasised that the working conditions of the social care sector have led to 74 per cent of care professionals reporting that they regularly experience stress at work, an average number of sick days 25 per cent above the national average, and a staff turnover rate significantly higher than the national average.
As phrased by one participant, social care is suffering from a “fatigued workforce” not only due to the pressures of the pandemic, but issues which have existed within the sector for much longer. The problems within the social care workforce are chronic , and are considered by many to constitute a crisis. As one participant said, “clearly a workforce strategy is one of the absolute essentials that we need to have to make a success of the sector over the next decade or so”.
“The social care sector should work alongside recruitment organisations to recruit young, bright people into social care, and help them consider where a career may lead.”
One problem identified was narrow recruitment to the sector. It was stressed that within social care, “we should cast our nets wider in a recruitment approach… and recruit not only people with previous experience”. The social care sector should work alongside recruitment organisations to recruit young, bright people into social care, and help them consider where a career may lead.
It was also suggested that more effort must be made to recruit hard-to-reach and underemployed groups, including people living with disabilities, and immigrant workers. “What frustrates me is that there are individuals in these groups who can be wonderful, caring staff [but]are missed, because hiring managers are too narrow in their focus”, said one participant.
Staff retention rates in social care are low. Network members noted that social care workers often leave the sector for other, similarly paid jobs, such as retail roles, while few choose to leave and work for the NHS. One network member identified that “between care assistants in the NHS and the social care sector, there is around a 23 per cent deficit in social care. The terms and conditions are vastly better in the NHS. Pensions, sick pay, overtime and unsocial hours all contribute to that deficit.”
Essentially, social care workers are underpaid and undervalued. For both better recruitment and retention, social care workers must be appropriately paid and treated as though they are valued. Some network members identified low pay as the key driver for individuals choosing to leave the social care workforce, and yet, it was emphasised that social care is a both a skilled and psychologically demanding profession, and should be commensurately well-paid.
However, funding in the system is limited, and paying the workforce is the sector’s single biggest expense. One participant said “there is not a settlement from government or local government that actually meets the cost of care to enable us to pay a proper wage for the level of skill, ability, responsibility, dedication that [care workers] have”. Furthermore, a high proportion of social care workers are on zero-hours contracts; in London, this figure stands at 41 per cent of social care workers. Therefore, many social care workers have to deal with pay inconsistency and insecurity, on top of being low-paid.
“Network members were in agreement that social care is, and should be publicly regarded as, a skilled profession.”
While pay is regularly described as the most pressing issue in the workforce, one participant argued that in their experience of conducting exit interviews with workers, it is not low pay, but rather a low sense of worth which leads people to leave the profession. While higher pay is one way in which care workers can be practically appreciated, it was agreed that more must be done to value care work both by improving the public image of care workers and ensuring that internal structures provide support and give value to workers.
Network members were in agreement that social care is, and should be publicly regarded as, a skilled profession. “It is not the kind of job that everyone can do,” said one participant. “It is a skilled job, which requires the creation of quality human relationships and working with people who have complex care needs… it is a real skill and should be regarded as the same as working in health.”
Social work is challenging and worthy of respect, all participants agreed. One commented that “no two days in social care will be the same; you have to be agile and move with that, so it does take very special people to take those roles”. The public status of social care work must be elevated to reflect this, and the workforce to feel appropriately valued if these retention issues are to be effectively addressed.
Securing an integrated future
For a supported workforce, good leadership is essential. One participant noted that in the social care system “there is a varied approach to leadership”, and good leadership is not always evident in the system. Given the demanding nature of social care work, it is essential that carers feel well supported in their roles. One participant added that “workers do not stay because of a good job, they stay because of a good manager”, and therefore, proper leadership training must be a central goal of the workforce plan.
A practical solution suggested by one of the network members to combat low recruitment, retention and the poor image of the profession was a ‘social-care-first’ scheme, mirroring the successful teach-first scheme. Many other sectors have emulated the ‘teach-first’ template with great success. The aim of the scheme is to engage with young people to consider social care work as a career by espousing the value of a career in care. Such a scheme would emphasise how care work has the potential to transform the lives of dependent individuals, and the importance and value in building personal relationships with system users, improving the image of the profession. As part of the scheme, there should also be structured leadership, coaching and mentoring training, for the purpose of also transforming the quality of social care. This may serve to solve some of the leadership issues in the sector, as young and bright individuals will be well trained to manage and lead social care in the future.
Now that the NHS and social care are moving towards integration, participants noted that for a true and fair integration of the systems, employees should be paid and treated equally. One participant called for a joint recruitment scheme for the NHS and social care, with equal pay offered. It was also emphasised that NHS workers receive many ‘perks’, particularly since the start of the pandemic, which social care workers do not (including food and drinks discounts from certain companies).
Other suggestions to aid the integration of the NHS and social care workforce included social care placements and secondments for NHS staff, in which they are exposed to social care, and the richness and value of social care work. The status of care work must be elevated for proper integration of the two systems can occur, in order that social work and NHS work can be equally respected.
A large part of the discussion focused on the role of volunteers within the social care sector, and the value they bring to both paid carers and system users. Volunteers are an invaluable part of the social care workforce given that they reduce pressure on care workers, improve patient experiences, facilitate higher quality of care to drive better health outcomes, and strengthen community connections. One participant said that in the context of social care, “volunteering is a public health tool. There is a body of medical research which talks about the huge benefits for mental health and physical wellbeing for patients”. Volunteers also serve to raise the visibility of the social care sector.
Since the start of the Covid-19 pandemic, the UK has seen an unprecedented rise in the numbers of people volunteering in their local communities. During the pandemic, the UK had 12.4 million people volunteering in their local communities. 4.6 million of these were first-time volunteers. Currently, the UK has a window of opportunity to make the most of the interest in volunteering to reduce the immense pressure on care workers.
As part of the workforce strategy, there needs to be investment to drive the volunteer sector, for the wellbeing of the social care system and its users. However, time is undoubtedly of the essence; as one participant emphasised, “there is an urgency to the conversation we are having. As Covid dissipates, what we don’t want is for people to go back into the corners of their community and not come out again to contribute.”
Spring Statement 2022: Key takeaways for health and care
By Gabriel Blaazer
While many of the measures in Rishi Sunak’s statement were welcomed, health leaders warn the government must go further to safeguard public health amid a spiralling cost of living crisis.
The Chancellor delivered his Spring Budget to the House of Commons today, in a statement dominated by events in Ukraine and the rising cost of living crisis. While there was little mention of health or social care directly, several measures announced pose significant implications for the health of the nation and the NHS workforce.
There was welcome relief for many of the lowest-paid, as the government announced the raising of the NI contribution cap by £3,000 (rather than the £300 initially suggested), from £9,500 to £12,500. According to the government’s own figures, this will take around 2.2 million people out of contributing to the Health and Social Care Levy entirely. Some 50,000 businesses (those who employ four or fewer people) are also projected to become entirely exempt from the contribution, thanks to an increase in the Employment Allowance.
Although welcome to those continuing to be hit by the cost of living crisis, these tax cuts represent an annual £6 billion reduction in treasury tax receipts. With the Health and Social Care Levy initially aimed at raising £11.4 billion a year over the years 2022-2025, the details of the Spring Budget seem to imply a 52 per cent reduction in that figure, at least in the short-term.
In mitigation, the government also announced “that it will double the NHS efficiency target from 1.1 per cent to 2.2 per cent a year, freeing up £4.75 billion to fund NHS priority areas over the next three years, and ensuring that the extra funding raised by the Health and Social Care Levy is well spent.”
Mr Sunak also announced a 5p per litre cut in fuel duty, a move that will benefit healthcare staff, such as district nurses, physiotherapists and midwives, who rely heavily on their cars to deliver domiciliary and community-based care. The cut, however, falls short of action called for by the NHS Confederation and NHS Providers in a recent statement.
Health leaders welcome tax cuts but call on government to do more
Responding to the Chancellor’s Spring budget, NHS Confederation Chief Executive, Matthew Taylor, said: “Health leaders broadly welcomed the additional funding for health and social care in the Chancellor’s Budget last October and recognise the importance of putting this investment to best use but the world around us is very different now.
“This comes as the NHS is already operating with reduced capacity, very high bed occupancy, and 110,000 vacancies, which will compound how much its services can identify further efficiency gains. Also, our members are very concerned by how hard individual NHS staff members will be hit by this cost-of-living crisis.
“A concession has been made in the fuel duty reduction, but we need to see the Treasury go further to shield community-based healthcare staff from soaring prices at the pumps as they rely on their cars to see their patients, including those who are housebound. A lot is uncertain but as the cost-of-living impact bites the Chancellor must be live to the increased strain and pressure it will put on the NHS in his next Budget this autumn.”
Nigel Edwards, Chief Executive of the Nuffield Trust, said: “Amid a cost of living crisis, it is not surprising that the Treasury will be scrutinising the increased spending on the NHS raised by higher taxes and looking for cost efficiencies.
“Changes to national insurance threshold announced today will provide some welcome support to low earners and will not reduce the amount of money already committed to health and care. But by choosing to put tax cuts above spending the Chancellor has made it less likely that health and care will see any further increases in funding during this parliament.
“This underlines that, despite a boost from the levy, the NHS will still face tight budget constraints. Funding increases to the NHS’s core budget become less generous in each of the next three years, which is why the Chancellor has doubled the annual efficiency target to 2.2 per cent. In reality, however, NHS trusts will need to find even more room for efficiency than that, as at the same time there will be steep reduction in Covid support despite the fact this cost pressure is likely to remain in place for some time yet.”
Jo Bibby, Director of Health at the Health Foundation said: “Today’s announcement shows that the government has yet to fully grasp the pandemic’s stark lesson that health and wealth are fundamentally intertwined. Despite the measures set out today, household incomes are set to fall by 2.2 per cent in real terms in the coming year.
“The pandemic has stretched the financial resilience of many families to its limit. Many have run down their savings or increased debts to cope with the impact of Covid-19 and measures to contain it. And there is no sign that there will be any let up with CPI inflation set to peak at 8.7 per cent at the end of the year. This continuing rise in cost of living will force increasing numbers to choose between essentials that are vital to living healthy lives – such as housing, heating, and food – or being driven into problem debt.
“A government that truly valued the nation’s health would have gone further today to protect the most vulnerable families from this latest economic shock. The increase to National Insurance thresholds is significant but fails to target the poorest households. There has been no action on benefits, while the additional £500 million for the Household Support Fund falls well short of what is needed. Higher inflation will also erode planned spending on public services which support health. The government should be investing more to protect people in the here-and-now, as well as building greater resilience against future threats to our health.”
How integrated care systems can improve digital inclusion
By Gabriel Blaazer
Sarah Boyd, Head of Digital Experience and Transformation at Norfolk & Waveney Health and Social Care Partnership (NWHSCP), explores how her integrated care system (ICS) is using digital health to improve patient inclusion and help reduce health inequalities.
Health inequality is a growing problem but is still too often discussed separately from the core business of the NHS. Patients are treated through siloed care pathways, with conversations about why some populations have poorer health outcomes often treated as an aside.
The pandemic brought this into greater focus, especially around digital inclusion. Technology rolled out across the NHS in response to Covid-19 often widened the gap between those who could access online services and those who couldn’t.
The benefits of ICSs
When it comes to digital inclusion, there is little doubt that ICSs offer a huge opportunity to deliver more equitable access to healthcare and improved health outcomes for those previously underserved by the health system.
NWHSCP is a new type of organisation, working as a system across the Norfolk and Waveney region. Operating across the public sector, along with health and social care, councils and with voluntary organisations, presents an opportunity tackle health inequality and exclusion in a person-centred way.
The ICS allows health leaders to work across organisational boundaries, to test assumptions about exclusion, and to leverage the work that happens at the level of individual places.
Fixing existing digital inequalities
At every stage, NWHSCP are ensuring that their digital projects address digital inequalities. By implementing a pan-public sector hub-and-spoke model that provides personalised support to excluded groups, their plan is to gain the wider benefits of digital inclusion by engaging people – not only in health services – but more broadly in society.
For example, if a GP detects that an elderly person in their care is socially isolated, they can refer them to a central digital inclusion service. From there, they may be passed to a library or volunteer service who are able to provide connectivity or a 5G-enabled device, along with the ongoing support to use it. This allows the patient to order repeat prescriptions, but also to food shop online or video call family and friends, with positive benefits for their wider health and wellbeing.
“Creating an environment in which every service is digitally inclusive offers benefits not just to individuals, but also to wider society”
Asking people to go to an appointment at an unfamiliar location can create unnecessary barriers. As it proceeds, the ambition of NWHSCP is to work towards using services that people already access to provide a trusted contact point. If patients are already known to a church group or domestic violence shelter, for example, they might receive support there.
Through community partnerships, ICSs can build a network of digital tools and skill provision. For example, if a partially-sighted person, or family member, needs a speech-to-text reader, NWHSCP can point them towards their trusted toolkit. Once a person has access to this network, they can then download tools freely, ahead of their health needs.
Building an inclusive service
Creating an environment in which every service is digitally inclusive offers benefits not just to individuals, but also to wider society. As the Good Things Foundation’s Widening Digital Participation report found in March 2020, digital inclusion pays for itself in better mental and physical health, and stronger participation in the economy. For every pound spent, £6.20 is made back.
With this in mind, ICSs can leverage skills found in the private sector to identify new ways to increase inclusivity. Companies in the space include ThriveByDesign and CardMedic, an award-winning digital tool that provides instant access to communications options to improve engagement with healthcare professionals.
CardMedic is designed to help patients with a language barrier, visual, hearing or cognitive impairment, or to communicate through PPE and is unique in its space.
One issue with digital inclusivity tools is that they’re often seen as only affecting excluded communities, but digital inclusivity applies to everyone. Many people often struggle to retain emotionally-sensitive medical information, such as details about a cancer diagnosis. Tools like CardMedic allow any patient to review the basics of a hospital procedure or consultation – helping them to feel more secure in their care.
Applying innovation
Through pulling together with public sector and voluntary organisations, NWHSCP has built a strong, interconnected and multi-disciplinary team to implement their digital transformation agenda. As ICSs move towards statutory footing, the hope is to build on their initial successes though good recruitment and the implementation of innovative technology.
But there is only so much one system organisation can achieve on its own. To maximise the potential of integrated care systems, the NHS will require a national system for picking up on digital innovation. It should not be up to individual ICSs to find products, such as CardMedic, themselves. Digital inclusivity should be available to all.
Taking practical steps to address a growing crisis in domiciliary care
By Gabriel Blaazer
John Bryant, Head of Strategy and Development for Torbay Council, outlines a series of practical steps to enhance the role of the care worker and address the growing crisis in domiciliary care.
The solution to the domiciliary care crisis is to enable the sector to do more, not to simply ask more of it. The distinction is important, as the development of integrated care provides opportunities to enhance system efficiency like never before. And yet, the scope of what could be asked of, and performed by, trained, supported, committed community-based practitioners is yet to be fully explored or achieved.
All the while, the expectations of those receiving care, and certainly those considering a future career in health and care, are greater than they have ever been.
To meet these ever-rising expectations, system leaders are likely to find fertile ground in looking to better embrace the assets that already exist within the system. This includes domiciliary care workers, whose skillset could be expanded and developed, a move that could encourage others into the system. This can happen by re-positioning the expectation, skills and rewards to produce and provide, for example, enhanced wellbeing services (EWS) provided by enhanced wellbeing practitioners (EWP), of which domiciliary care is a major component among a portfolio of beneficial interventions and service provision.
The 6Cs of care are prevalent within our frontline domiciliary partner staff; the opportunity is there to optimise their engagement and knowledge of patients and clients to:
Support retention and recruitment
Respond to the discharge and reablement challenges
Drive early intervention and prevention
Offer a developed interface with general practice
Engage with population health management
The support of these four key drivers for public service change: politics, policy, measurement and money, are positioning us as never before to achieve success. The government’s social care reform white paper, People at the Heart of Care, connects to the £5.4 billion pledged for adult social care reform between 2022 to 2025. It is notable that healthcare is a major beneficiary of this funding in early years, however within the policy of integrated care the opportunity exists to bring about radical, beneficial system reform from the outset.
“Together, these measures aim to put people at the heart of social care and move us towards our 10-year reform vision.”
(Department of Health and Social Care, 2022).
These themes were also present in the subsequent integration white paper, Joining up Care for People, Places and Populations. The measures set out in the paper provide clear areas of opportunity, focus and policy support.
A growing crisis
These government white papers are in no small part a response to a care crisis the likes of which we have never seen. One key element of that is domiciliary care, the unseen service that is delivered behind the front doors of our communities to keep people safe, comfortable, medicated and cared-for. For over a decade the policy has been to bring care closer to home, and the People at the Heart of Care paper reinforces that. The Covid-19 pandemic has compounded the need to ensure people are cared for and supported in this way, minimising their movement between different health settings to reduce infection risk.
“The endeavours of care providers to recruit at this level should be celebrated alonside any other part of the system that has been able to do the same”
Present estimates indicate that there is a care shortage/vacancy rate of 17 per cent which equates to at least 100,000 jobs based on Skills for Care data in England. Given the challenges in recruitment felt by providers, there can often be a projection that care providers are not ’good‘ at recruitment. However, in looking behind the headlines we find that in one area, Torbay, care providers have increased their capacity through recruitment by 39 per cent in the 18 months leading to September 2021. The problem is that the demand for their services has totally outstripped this staffing influx, increasing by 47 per cent in the same time period. This trend is consistent across the country’s health and care ecosystem.
The endeavours of care providers to recruit at this level should be celebrated alongside any other part of the system that has been able to do the same. If organisations who have been able to recruit as well as Torbay have done are finding it difficult, is it probable that any other part of the system will do better?
The Health Foundation recently published research suggesting that over a million more health and care staff will be needed in the next decade to meet growing demand for care. What is clear is that these shortages were well established trends before the Covid-19 pandemic. If the challenge of capacity is to be permanently addressed, then retention followed by recruitment is essential – as any marketing of roles from ‘the system’ will be trumped by the messages communicated by those working in or leaving the services.
Recognising a new future, communicating that and providing examples of what could be achieved will produce opportunities for beneficial results.
Practical steps
In this respect, returning to the domiciliary care issue, what might emerge if we were to turn the issue on its head?
To address the crisis currently seen in domiciliary care, I propose a series of practical steps to enhance the role of the care worker and to use the ICS framework to transform system level efficiency:
Addressing the domiciliary care shortage: expand the potential of the service and provide those delivering it with more responsibility and control by becoming EWPs
Supporting the community nursing challenge: offer them the opportunity to have a wider team of EWPs at their disposal; enable them to work to the top of their licence
To address GP availability: create neighbourhood teams of EWPs that are able to be with patients, directly support with digital literacy and connectivity, and be a physical presence to further enhance the experience of the remote general practice
To reduce A&E admissions and improve the discharge process: use EWS to support the safe discharge of increasingly complex patients to optimise recuperation in at-home settings, have the digital skills and tools to monitor and report e.g. RESTORE2 for early intervention and re-admission avoidance, and be able to support reablement; the stepping stone to independence
Develop greener care:reducing mileage by minimising cross-overs between staff and building a wider multi-disciplinary team
The practical possibilities for this are supported by the further development of the Allied Health Professionals strategy. The publication of the Allied Health Professions’ Support Worker Competency, Education and Career Development Framework received support from Trades Unions, Professional Bodies and Trade Union partners. Whether it is development within roles or providing new career paths, new forms of offer and opportunities are going to be central in encouraging a post-Brexit, domestic workforce into the social care and health sector; along with producing the impact value of those roles and associated care interventions which enable commensurate levels of pay and reward.
Underpinning all endeavours and quality care and support are the 6Cs of Care. These emerged as part of ‘Compassion in Practice’ and were rolled out by NHS England to all staff in 2014 with subsequent promotion to the wider care sector by the national body Skills for Care.
“But what cannot happen is that domiciliary care continues to be overprescribed without receiving more support or being allowed to expand its offering”
The characteristics of commitment, care, compassion, competence, communication and courage are prevalent throughout our community care partners and their staff. With that commonality between the professions what might we do to deliver even more fulfilling roles: more people doing fulfilling roles, more fulfilment within the roles, more roles in addition to the present ones that are also fulfilling?
The alchemy that will bring this about is within the gift of every system in England and available to all domestic nations. It is the meaningful flourishing and delivery of an integrated care system (ICS). The ‘holy grail’ of ICS development is to provide timely, personalised care that maximises the independence of the individual receiving care which, naturally, points to a home-based solution. But what cannot happen is that domiciliary care continues to be overprescribed without receiving more support or being allowed to expand its offering.
This article seeks only to look at one small area of that; however, it is a vital area, being felt by the 957,000 people in the UK that receive domiciliary care and their families, along with the 822,000 staff looking after them (as recorded by RCN surveys). This, quite rightly, is now receiving both political support and national media attention.
The pandemic should be recognised as a catalyst for accelerated change, avoiding any sense of ‘once we’re through this we can get down to business as usual’. What has been done, and is being done in response to the pandemic, has demonstrated the creativity and pace of change possible as system partners have collaborated. Fostering and building on that is in itself both an opportunity and a challenge.
Across the sector there are understandable concerns of implementing radical service reform on an already exhausted and beleaguered workforce. But there are examples we can look to where workforce wellbeing is protected while simultaneously enhancing capacity and quality of care that motivates staff.
Some facts from one system
To service 800 clients in a 75-mile geographical perimeter, home care staff drive almost one million miles per annum. In work supported by the Health Foundation, it was found that at a (sub)urban travel speed averaging 20 mph, over 43,500 hours were being spent in vehicles; a substantial proportion of that could be put to new ways of working.
Work has shown that by reorganising the rounds, 5,220 hours of care could be released from the existing workforce. This would provide opportunities not only for more care to be delivered but importantly, and in respect of future retention and recruitment across the system, time for wellbeing, supervision, learning and development, accreditation of skills and assurance in their application. And with no extra hours of care being purchased.
In terms of application and the development of broader multi-disciplinary teams within ICSs, it was established that of the community nursing patients nearly 20 per cent were also social care clients. People were being visited by multiple staff in one day, requiring travel from multiple staff.
There are of course many activities and health interventions which can only be done by those with nursing and clinical qualifications. However, in approaching this issue with a mindset of curiosity, courage and compassion there are many interventions that could be performed in different ways.
For instance, one of the many activities that domiciliary care staff undertake is washing and creaming clients’ legs when there are wounds to be attended to. Nursing staff will then arrive to apply a bandage. While certain grades of wound clearly need nursing attention there are many at lower levels of severity that are capable of being attended to by a well-trained EWP – and of being checked on regularly, though less frequently, by the stretched community nursing complement.
Benefits of EWS for participants and for system development
Enhanced wellbeing practitioners:
Feel respected and able to develop their domiciliary care roles, feel even more a part of the system and that their contribution is valued. This could lead to enhanced profile and esteem. The additional activity means more time with the client and the opportunity to further enhance the relationship that exists
Opportunities will be presented to work in strengths-based ways and with programmes such as Making Every Contact Count, leading to enhanced wellbeing of the clients and a development of their connectivity and circle of support
This leads to improved job/role satisfaction – improved retention leading to increased recruitment. Developed circle of support for clients, enabling them to step up towards independence and reduce their reliance on statutory interventions. Release of capacity for those with assessed needs to have their needs met and begin their journey towards well-being
Community nurses
Feel an increased level of support with a bigger, more integrated, team available to them. They are then able to work with the more complex cases and make the very best use of their skills and knowledge while enabling and supporting other integrated team members to develop
Through enabling better management of case-loads, job satisfaction is increased and stress is reduced. As the RCN has established, with 75 per cent of community nurses reporting that they had left necessary activities undone, the professional dissonance of the role is alleviated, supporting staffwellbeing and retention
With the nursing and Allied Health Professional colleagues active in this way, early intervention and reductions in exacerbations of conditions lead to reduced admissions. With greater capacity, along with the skills to manage more complex discharges, hospital flow is improved
Benefits of EWS for health providers
Admissions through A&E:
Are reduced by earlier interventions and the ability to deploy the highly skilled staff in the community to support patients and reduce the deterioration in their condition
Improved flow through A&E with reduced admissions, enhancing the wellbeing of staff as well as the patients, and contributing to the enhanced application of funding to meet elective care
Discharges and re-admission rates:
Are further improved with the skills and capacity made available to support increasing numbers of and increasingly complex patients. With the integrated approach to working and early intervention opportunities, people are supported to remain at home, with their condition even better managed and do not require a re-admission to hospital
Skills and capacity across the community integrated team are available to support timely, safe discharge from hospital and discharge to assess and ensure people remain at home
The patient/client gets less ill and recovers more quickly being supported by a team that has the resources, capacity and skills to meet their needs. This increases the ability for them to remain well or recover quickly in their home setting, which include care homes and supported living
Increased numbers of people cared for closer to home with reduced exacerbations in conditions. Complex clinical requirements being met in community settings with both care-giver and the patient having a well developed strengths-based relationship throughout the care and support period, enabling a step up to independence
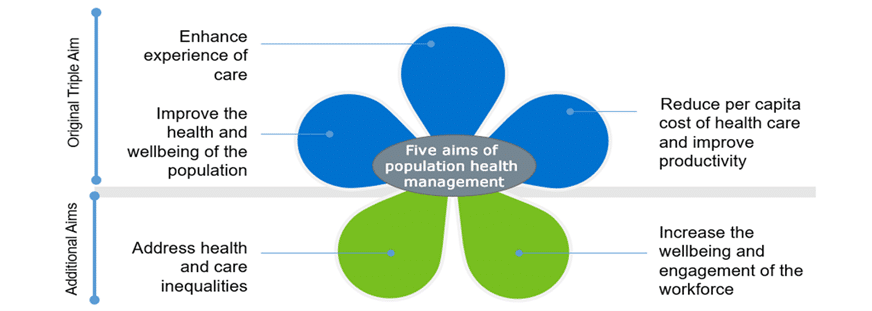
It is understandable that there will be anxieties associated with the shift in activities. In order to ascertain who delivers what and where to achieve the five aims of population health management (as illustrated below), the mantra to hold onto is right person, right care, right place, right time. Risk-managed prototyping using good design methodologies is key and implicit within the title on the tin of sustainability and transformation partnerships (the predecessor to ICSs).
There are many practical examples already available and still plenty of headroom for further development, which will accelerate the transformation in health and care models which are both sought for and needed.
Covid has shown us how much can be done in a short space of time; even with all the pressures in the system, GPs, acute trusts, AHSN and domiciliary care providers worked together to train 148 staff in the RESTORE2 methodology in just three months, with some going further to be trainers themselves.
Practical steps to developing and implementing enhanced wellbeing services
Train domiciliary care and care home staff to use the protocols and develop relationships with primary care practices
Ensure that training is accessible and that the nursing staff are corporately supported in the delegation of tasks
Look to see if care packages are allocated by geographically focussed provider or on first-come-first-served basis, and what the mileage component to the care rounds is for providers
Review the wounds being attended to in community settings and what best practice can offer in tackling the £5 billion cost of wound management
Consult on ways in which the Allied Health Professions’ Support Worker Competency, Education, and Career Development Framework can be optimised
Get the best facilitators and design thinkers, often found outside the system, to help ask the questions, listen and gather the answers and develop action-orientated plans with system partners – which includes the care unit, the patient/client and those caring for them
Whichever of the four policy drivers (politics, policy, money or measurements) one wishes to consider, they are captured within the Five Aims of Population Health Management; moving to EWS and development of the practitioners supports their delivery. Beyond this the one element that is maybe more implicit within the ‘petals’ below is capacity. EWS supports this explicitly.
Achieving more with less
In summary, below is the 30-second elevator review of how we can achieve more with less on the topic of domiciliary care.
More:
Time to care, more time to be more caring
Development and enrichment of roles
Person-centred care
Satisfaction with the role
Retention
Recruitment
Prevention and early intervention
Less:
Dissonance in the role and 6Cs
Siloed working
Variation in care team and discontinuity of care
Dissatisfaction with roles and system design
Turnover and leaving before retirement, or at the earliest opportunity
Vacancy and cost to trying to encourage people into services
Illness and cost
Addressing the care crisis
With the job-seeking public indicating that insufficient numbers of them wish to work in domiciliary care, now would be the time, supported by the policy of integrated care, to develop a new offer that enables truly integrated roles. This should seek to provide enhanced wellbeing services through an increasingly broad, multi-disciplinary, person-centred team.
To address this multifaceted care crisis, we should do more than seeking to invite people into traditional domiciliary care. The system might benefit from offering people a new role(s) that encompasses the domiciliary care that they are proud to already be doing, but also one that offers development, inclusion, satisfaction, esteem and commensurate compensation. This could become increasingly available if and when ICSs fulfil the potential that exists; one that reflects those stated aims within the recent white paper(s) and meets the five tenets of Population Health Management.
This should also note the observations of the CQC and their likely support to engage in discovery sessions for regulation alignment towards new ways of working. In doing so this should create a virtuous cycle towards a sustainable system, both financially and with capacity, through the delivery of integrated care.
John Bryant is Head of Strategy and Development for Torbay Council and an ICJ contributor. To contact John, become an ICJ contributor or to obtain a full reference list for this article, please write to news@integratedcarejournal.co.uk, and one of our Editors will assist.
PPP calls for adequate social care funding to end postcode lottery
By Integrated Care Journal
Public Policy Projects (PPP) has launched its first Social Care Network report, Mind the Cap: choices and consequences for financing social care, addressing the need for radical financial restructuring within the UK social care system.
The report, launched on 14 March, finds that the standard and financing of social care in the UK is subject to a postcode lottery. Given that social care is funded locally, there is vast regional inequality in the standard of care in the country.
Even with some level of means-tested support, and the newly introduced cap, the PPP Social Care Network found it a system unaffordable for many. The report concludes that these measures do not protect some low-middle income households from having to spend entire savings on social care.
PPP brought together 25 senior stakeholders and experts within the sector to discuss solutions to the crisis ahead of the spring budget. The report is sponsored by Radar Healthcare and the Royal Voluntary Service.
In September, parliament agreed to increase National Insurance Contributions by 1.25 per cent to establish a new ‘Health and Social Care Levy’ and introduced a new measure to cap care costs at £86,000. However, only a small proportion of money generated by the levy will go to social care, and the cap does not protect low-middle income individuals or families.
PPP’s social care network find that the Levy proposed by the government will not even begin to address the costs of care required by the system, and the cap protects those who are least likely to use the system.
Speaking at the report launch event, former Deputy Prime Minister Damian Green, said: “The current Health and Social Care Levy falls on the working age population, all of whom will be faced with inflationary cost of living pressures which we haven’t seen since the 1970s. It is falling on a particularly vulnerable portion of society.”
Key recommendations from the report include:
The government must focus its attention on how best to stimulate a wider insurance-based approach to care, encouraging individuals to participate in voluntary insurance schemes to cover costs up to the cap
The government should widen the scope of the Health and Social Care Levy; other forms of income and wealth for which National Insurance does not apply, such as rental income for private landlords, should also be considered for a social care levy
The government should explore greater flexibility around the Health and Social Care Levy, including the option of directing a proportion of the levy to an individual’s social care insurance scheme and/or contributions being made up by employers, as with pension schemes
The report emphasises that there is insufficient funding overall in the sector and that local authorities and care providers must be adequately funded for any improvement of the social care system. It also outlines that this funding should come from both private payment and higher state provision.
Mr Green said: “The adequate financing of social care is vital for the proper functioning of the system. Once we inject an appropriate amount of money into the system which has, quite frankly, been on its knees for years, we will begin to see the problems of the social care system begin to melt away. The measures proposed by the government are not sufficient, and more must be done to support those in need of care.”
Commenting on the report, Dame Esther Rantzen, Broadcaster and Founder of ChildLine and The Silver Line, said: “I know how crucial adequate funding is, both for those who offer care, and for those who receive it. The caring profession needs far better funding to give carers the opportunities and status they should have and enable them to give their work the time and skill it needs. And vulnerable people who need support should not have to worry whether they can afford the right care. Without proper funding carers will continue to be undervalued and their work unappreciated when in fact more and more people depend upon it.”