Case study: Improving diabetes care in Norfolk and Waveney

How collaboration between DUET diabetes and Norfolk and Waveney ICB is helping to upskill healthcare professionals involved in conducting primary care diabetes reviews.
DUET diabetes was founded to improve the understanding and knowledge of those looking after adults with diabetes. The service offered is designed to improve the skills and confidence of professionals working in health and social care roles and the standards of diabetes care they provide; ultimately benefiting the people (adults) they look after.
DUET has been working with Norfolk and Waveney integrated care board (ICB) to develop a face-to-face workshop programme as part of their creation of a Diabetes Training Academy. Through the creation of a central diabetes training hub, the ICB aimed to:
- Drive excellence in diabetes care, ensuring healthcare professionals (HCPs) had the competencies they require to improve the management of diabetes.
- Reduce potential complications that arise from more uncontrolled diabetes.
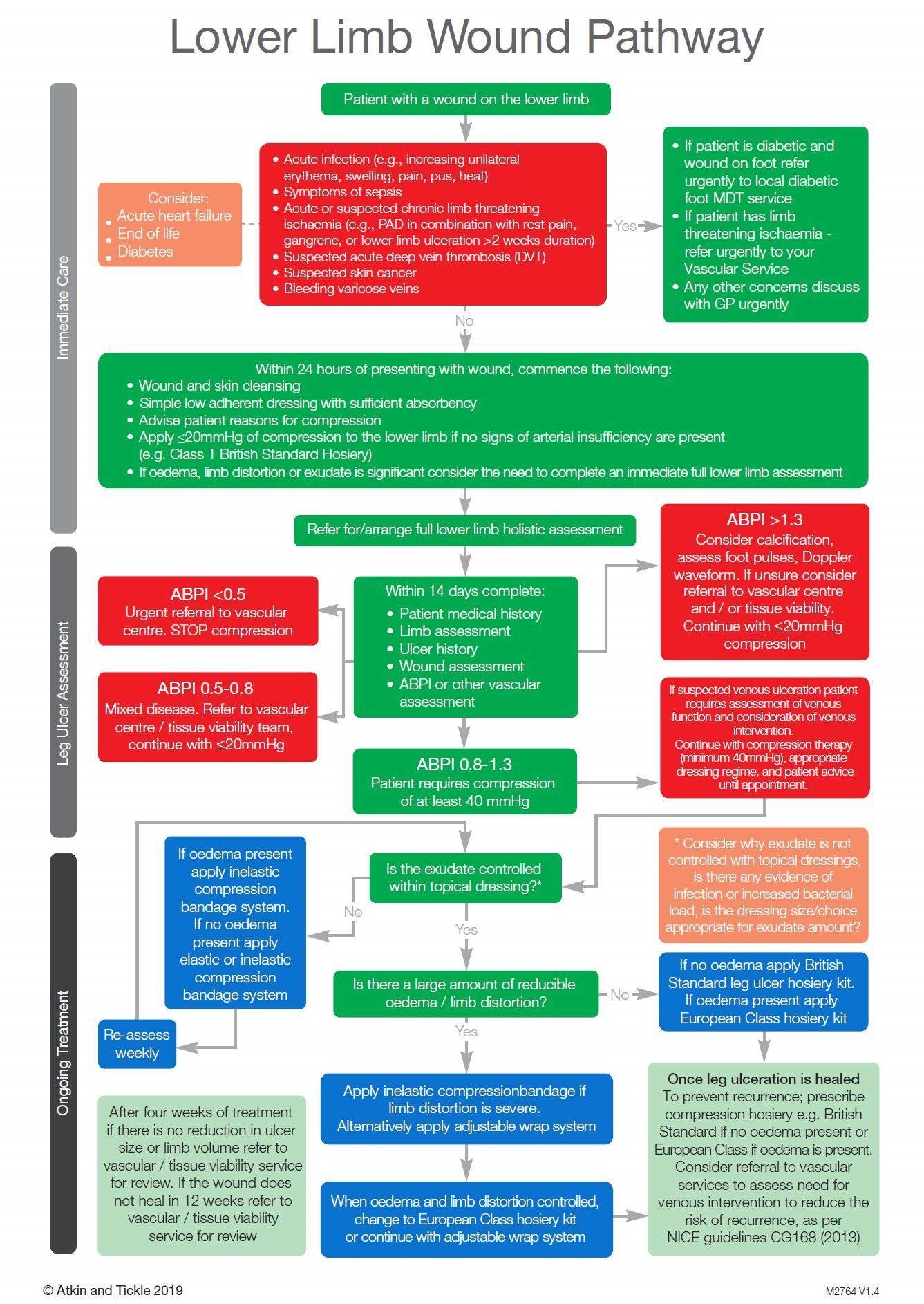
The workshop programme was designed for HCPs involved with conducting diabetes reviews within primary care practices. The content focussed on laying the foundations of understanding diabetes and its management and then built upon these to include the ‘eight key care processes’ and the importance of a ‘holistic diabetes review’. A key aspect was to ensure that learners could confidently and competently undertake a diabetic foot screening examination and be aware of the local footcare pathways.
Representatives of the ICB involved with driving this initiative also attended the workshops to further understand the challenges taking place in primary care (looking specifically at local issues) as well as better understand the inconsistencies.
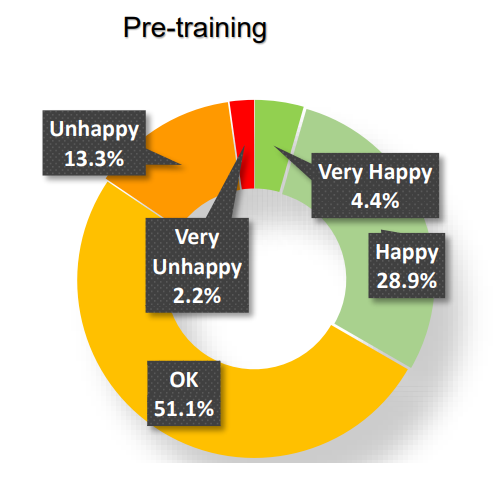
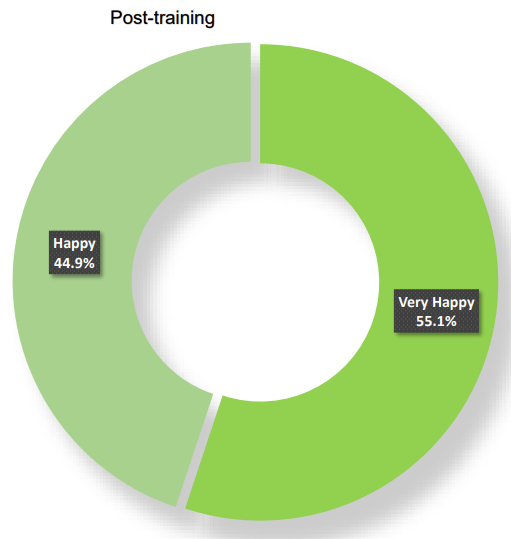
The workshops have been attended by 55 HCPs (additional funding is being sought to roll out further training), with overwhelmingly positive results:
- 100 per cent of learners recommended the workshops.
- 100 per cent also felt their knowledge and skills had improved because of the training.
- More than 80 per cent of learners indicated a preference for learning in small groups that are interactive and led by a professional.
- Fewer than 2 per cent indicated a preference for E-learning.
The training has helped HCPs to understand how to be more person-centred by understanding the impact diabetes can have; such as the importance of pre-conceptual care and availability of additional local services. Being better educated, knowing when and where to refer concerns, providing a person-centred, safe and responsive service enables HCPs to provide appropriate support (and education) to people living with diabetes in a caring and effective manner. The ultimate beneficiaries are the people living with diabetes.
“Very happy with this course! One of the best courses in healthcare I have done. I have learnt so much, and gained lots of confidence in diabetic reviews and foot checks.” Tiffany Ellis Healthcare Assistant, Primary Care
“It was a lovely small group and we all engaged in the activities, as well as ask and answer questions.” Sam Chapman Healthcare Assistant, Primary Care
![]()
For more information about DUET diabetes, click here.