Aligning value and incentives to make digital health really work

How can we bridge the gap between health and technology companies and the NHS? Professor Terry Young and Jacqueline Mallender ask what barriers need to be overcome to facilitate transformation in healthcare.
Why do Digital Health Technology (DHT) companies experience financial and operational barriers when launching their solutions to the NHS? After all, the National Institute for Health and Care Excellence (NICE) has made the UK a global leader in health value, while the NHS itself should be able to think and purchase as a single system.
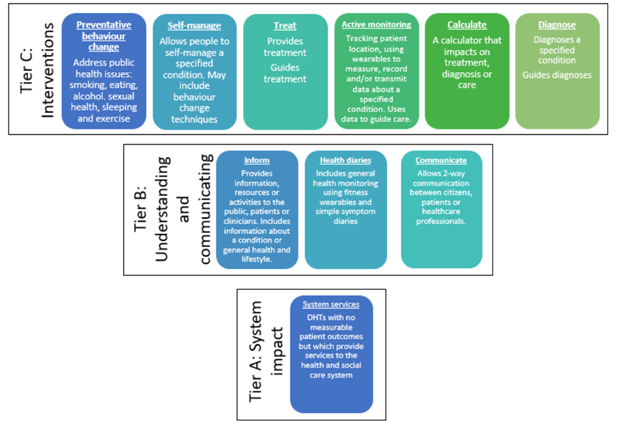
The NICE Evidence Standards classify technologies into three tiers of evidence according to their use, the highest burden of proof being required those which directly impact patient care, with the lowest being required for those focused on operational efficiency, as shown in Figure 1.
In reality, healthcare providers face operational and budgetary constraints which limit their ability to adopt solutions despite evidence of clinical effectiveness or economic benefit.
- NHS Finance Directors ask: “Can we afford this investment at this time for our organisation?”
- NHS Managers ask: “Can we manage and adapt our processes to fit this DHT into our operating procedures?”
Providers might understand the economic value and clinical benefits of a DHT, but this value may not resonate for a busy department with tough in-year efficiency targets and tight financial control totals to adhere to.
For example, there may be a strong economic case for investing in a DHT which improves the management of a chronic illness. The longer-term savings in treatment costs and the positive QALY (quality-adjusted life year) impact of better disease management, usually outweigh any additional input costs which might be incurred. However, if short-term investment is required and the department responsible for the relevant budget faces savings targets or in-year performance targets for existing processes, it may have neither the financial headroom nor the operational space to justify cuts elsewhere or to shift resources, even if this will improve clinical outcomes eventually.
Similarly, an investment may make financial sense for the hospital as a whole, but the clash between economic and business value may still prevent a finance director from cutting one departmental budget to invest in another. Moreover, the clash between clinical value and current operations may also stall DHT adoption, especially where there are competing demands on management time; and implementation may feel like one task too many.
Where an investment only makes financial sense for an entire health system, the problem is sharper still; cutting payments to one provider to create a new pathway in another is a big risk and faces considerable opposition from the “losing” provider, especially if the legacy assets and infrastructure still need to be paid for by someone. The alternative of securing extra short-term cash to fund the launch of new DHT can simply be too challenging.
A technology may cost more than the current standard of care but still be worth doing because of the positive impact on clinical outcomes. In such cases, the cost per QALY using that technology might be lower than the NICE implied threshold – and therefore good value for money. However, for DHTs which do not save money but provide much better health, it is pretty much “game over” for adoption unless the new technology is mandated.
What can be done?
At the national payer level, NHSX and NICE should continue to promote methods that highlight the benefits from all perspectives and provide national mandates for high-value DHT solutions which impact operational and clinical workflows respectively.
At the health system level, the move to integrated care systems (ICSs), integrated care providers (ICPs) and primary care networks (PCNs) and the new financial frameworks being applied, provides potential space for system-wide contracting advances. This is critical in the case of new DHTs where the benefits to the whole system are evident but no individual actor has the right financial incentive or operational space to move forward.
We would strongly encourage those supporting the establishment of these new systems to ensure the frameworks for making decisions have the sophistication and flexibility to identify such value propositions.
At the coal face, finance and management teams need to be rewarded rather than punished for taking business and operational decisions which improve whole system effectiveness and efficiency.
The impact of these clashes is easy to understand but reconciling the perspectives to make better decisions is very difficult and new methods need to be developed to make consistent decisions. Then, it will take courage to change things for the better.
About the authors
Jacque Mallender is an Economist and co-founder at Economics by Design. She is a respected international health and public policy economist and health evaluation practitioner. Over the last 35 years, Jacque has worked across health and social care with a focus on evaluation and health economics in UK, Europe, North America and more recently the Middle East and North Africa. She was a founding convenor of the joint Campbell and Cochrane Economics Methods Group and for 15 years was a committee member. In addition to her work at Economics By Design, Jacque is a Member of the Executive Committee of the Economic Research Council and an Associate of the Oxford Centre for Triple Value Healthcare.
Professor Terry Young worked in industrial R&D before becoming an academic and is now Director of Datchet Consulting. With over 30 years’ experience in technology development and strategy, health systems, and methods to ensure value for money, his current focus lies in designing services using computer models and he set up the Cumberland Initiative to support healthcare organisations wishing to develop their services more systematically.
Three of his downloadable papers are:
Using industrial processes to improve patient care (2004, with Brailsford et al., British Medical Journal)
Performing or not performing: what’s in a target? (2017, with Eatock & Cooke, Future Hospital Journal)
Systems, design and value-for-money in the NHS: mission impossible? (2018, with Morton and Soorapanth, Future Hospital Journal)